IRCCS Mondino Foundation, Genomic and post-Genomic Center, Pavia, Italy.
Unit of Medical Genetics, S. Anna University-Hospital, Ferrara, Italy.
J Headache Pain. 2018 Aug 30;19(1):75. doi: 10.1186/s10194-018-0891-x.
Familial hemiplegic migraine type 1 (FHM1) is a form of migraine with aura caused by heterozygous mutations in 4 genes: CACNA1A, ATP1A2, SNC1A and PRRT2, but further heterogeneity is expected. Here have been described clinical and molecular features in patients suffering from migraine with Aura (MA), without (MO) and hemiplegic migraine attacks. Next Generation Sequencing by TruSeq Custom Amplicon for CACNA1A and ATP1A2 gene has been performed. All genetic variants have been confirmed by Sanger sequencing and all samples were also analyzed with MLPA assay for ATP1A2-CACNA1A genes to detect duplication or deletion. All MLPA data were verified by Real Time PCR.
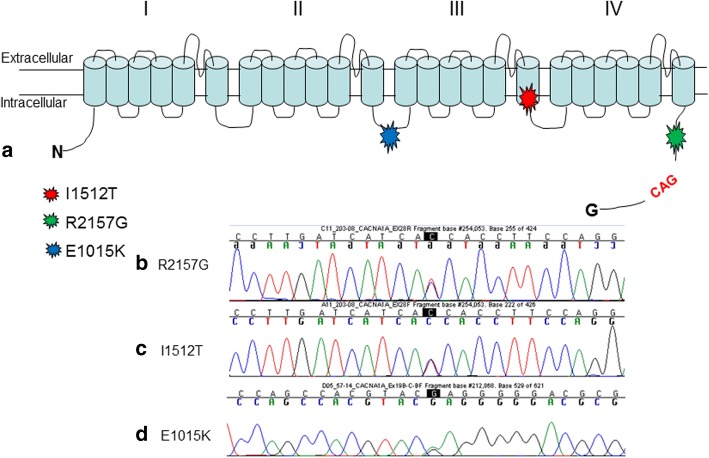
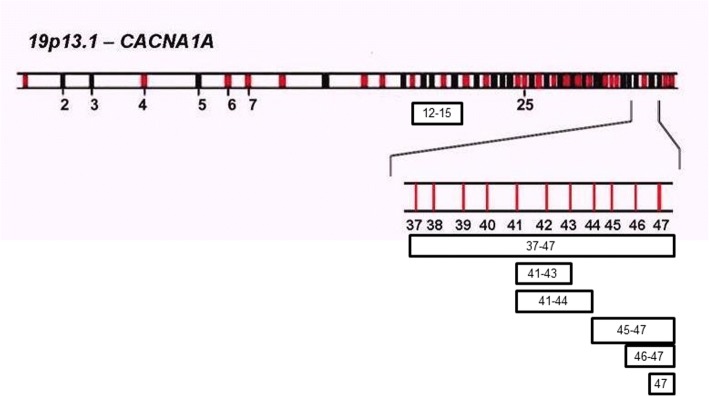
Sequencing analysis showed 3 point mutations, two novel variants and one already described in literature. Moreover, MLPA analysis showed 3 deletions in 9 sporadic hemiplegic migraine (18%), in 3 patients with non-hemiplegic migraine (4.1%) and in 3 patients affected by episodic ataxia (20%). Two sporadic patients showed a deletion in exons 41-43, while the rest of HM patients (5) showed a deletion in the terminal part of the CACNA1A gene. About episodic ataxia, we have identified deletions in exon 12-15 and in exon 47. Finally, in migraine patients, we have found different subjects affected by different phenotypes deleted in exon 47.
This work highlights the importance to complement analysis as direct sequencing with quantitative analysis (MLPA). In fact, intragenic CACNA1A rearrangements have been detected. Our work demonstrated that deletions in CACNA1A gene may be associated also to different migraine phenotypes.
家族性偏瘫性偏头痛 1 型(FHM1)是一种有先兆偏头痛,由 4 个基因的杂合突变引起:CACNA1A、ATP1A2、SNC1A 和 PRRT2,但预计还存在更多的异质性。本研究描述了患有偏头痛伴先兆(MA)、无先兆偏头痛(MO)和偏瘫性偏头痛发作的患者的临床和分子特征。对 CACNA1A 和 ATP1A2 基因进行了 TruSeq 定制扩增的下一代测序。所有遗传变异均通过 Sanger 测序确认,所有样本均通过 MLPA 分析 ATP1A2-CACNA1A 基因进行分析,以检测重复或缺失。所有 MLPA 数据均通过实时 PCR 验证。
测序分析显示 3 个点突变,2 个新变异和 1 个已在文献中描述的变异。此外,MLPA 分析显示 9 例散发性偏瘫性偏头痛(18%)、3 例非偏瘫性偏头痛(4.1%)和 3 例发作性共济失调(20%)患者存在 3 个缺失。2 例散发性患者表现为 41-43 外显子缺失,而其余 5 例 HM 患者表现为 CACNA1A 基因末端缺失。关于发作性共济失调,我们发现 12-15 外显子和 47 外显子缺失。最后,在偏头痛患者中,我们发现不同的患者表现出不同的表型缺失,缺失的外显子在 47。
本研究强调了直接测序与定量分析(MLPA)相结合分析的重要性。事实上,已经检测到 CACNA1A 基因的内含子重排。我们的工作表明,CACNA1A 基因缺失可能与不同的偏头痛表型有关。