Mercy Perinatal, Mercy Hospital for Women, Melbourne, VIC, Australia.
Department of Obstetrics and Gynaecology, University of Melbourne, Melbourne, VIC, Australia.
BMC Pregnancy Childbirth. 2018 Aug 31;18(1):354. doi: 10.1186/s12884-018-1992-x.
Fetal growth restriction is a disorder of placental dysfunction with three to four-fold increased risk of stillbirth. Fetal growth restriction has pathophysiological features in common with preeclampsia. We hypothesised that angiogenesis-related factors in maternal plasma, known to predict preeclampsia, may also detect fetal growth restriction at 36 weeks' gestation. We therefore set out to determine the diagnostic performance of soluble fms-like tyrosine kinase 1 (sFlt-1), placental growth factor (PlGF), and the sFlt-1:PlGF ratio, measured at 36 weeks' gestation, in identifying women who subsequently give birth to small-for-gestational-age (SGA; birthweight <10th centile) infants. We also aimed to validate the predictive performance of the analytes for late-onset preeclampsia in a large independent, prospective cohort.
A nested 1:2 case-control study was performed including 102 cases of SGA infants and a matched group of 207 controls; and 39 cases of preeclampsia. We determined the diagnostic performance of each angiogenesis-related factor, and of their ratio, to detect SGA infants or preeclampsia, for a predetermined 10% false positive rate.
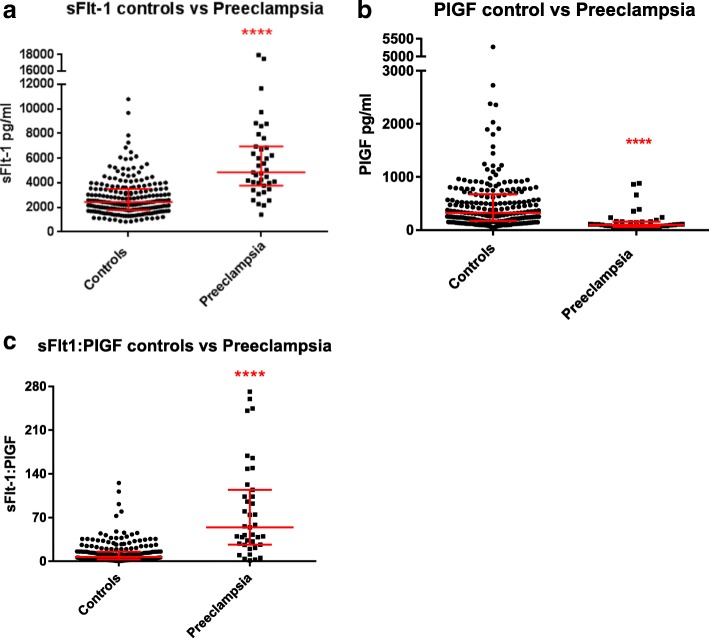
Median plasma levels of PlGF at 36 weeks' gestation were significantly lower in women who subsequently had SGA newborns (178.5 pg/ml) compared to normal birthweight controls (326.7 pg/ml, p < 0.0001). sFlt-1 was also higher among SGA cases, but this was not significant after women with concurrent preeclampsia were excluded. The sensitivity of PlGF to predict SGA infants was 28.8% for a 10% false positive rate. The sFlt-1:PlGF ratio demonstrated better sensitivity for preeclampsia than either analyte alone, detecting 69.2% of cases for a 10% false positive rate.
Plasma PlGF at 36 weeks' gestation is significantly lower in women who subsequently deliver a SGA infant. While the sensitivity and specificity of PlGF currently limit clinical translation, our findings support a blood-based biomarker approach to detect late-onset fetal growth restriction. Thirty-six week sFlt-1:PlGF ratio predicts 69.2% of preeclampsia cases, and could be a useful screening test to triage antenatal surveillance.
胎儿生长受限是一种胎盘功能障碍疾病,其死产风险增加三到四倍。胎儿生长受限具有与子痫前期共同的病理生理学特征。我们假设,在 36 周妊娠时可预测子痫前期的母体血浆中与血管生成相关的因子,也可能检测到胎儿生长受限。因此,我们着手确定可溶性 fms 样酪氨酸激酶 1(sFlt-1)、胎盘生长因子(PlGF)和 sFlt-1:PlGF 比值在识别随后分娩出小于胎龄儿(SGA;出生体重 <第 10 百分位数)的妇女中的诊断性能。我们还旨在在一个大型独立前瞻性队列中验证分析物对晚发型子痫前期的预测性能。
进行了一项嵌套的 1:2 病例对照研究,包括 102 例 SGA 婴儿病例和 207 例匹配对照组;和 39 例子痫前期病例。我们确定了每个血管生成相关因子及其比值在检测 SGA 婴儿或子痫前期时的诊断性能,对于预定的 10%假阳性率。
在随后分娩出 SGA 新生儿的妇女中,36 周妊娠时的 PlGF 血浆水平中位数明显低于正常出生体重对照组(178.5 pg/ml 比 326.7 pg/ml,p<0.0001)。sFlt-1 在 SGA 病例中也较高,但在排除同时患有子痫前期的妇女后,这并不显著。PlGF 预测 SGA 婴儿的敏感性为 10%假阳性率时为 28.8%。sFlt-1:PlGF 比值在子痫前期的检测中优于单独的分析物,10%假阳性率时可检测到 69.2%的病例。
在随后分娩出 SGA 婴儿的妇女中,36 周妊娠时的 PlGF 血浆水平明显较低。虽然 PlGF 的敏感性和特异性目前限制了其临床转化,但我们的研究结果支持基于血液的生物标志物方法来检测晚发型胎儿生长受限。36 周的 sFlt-1:PlGF 比值可预测 69.2%的子痫前期病例,可能是一种有用的筛查试验,用于产前监测的分诊。