Department of Surgery, Division of HPB and GI surgery.
Departments of Pathology and Immunology.
Am J Surg Pathol. 2018 Nov;42(11):1480-1487. doi: 10.1097/PAS.0000000000001144.
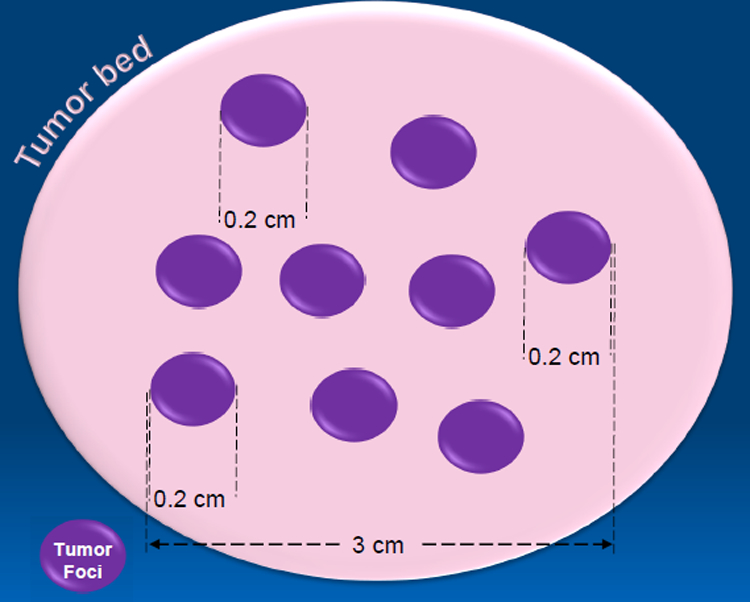
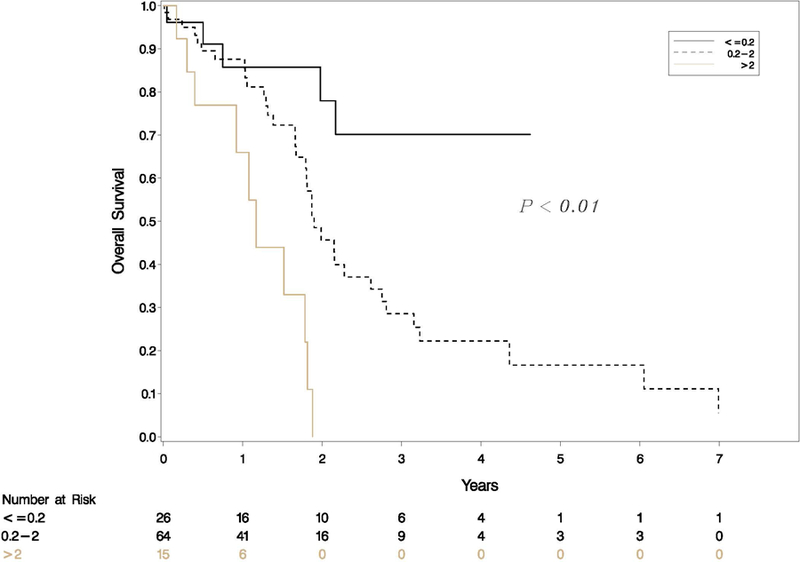
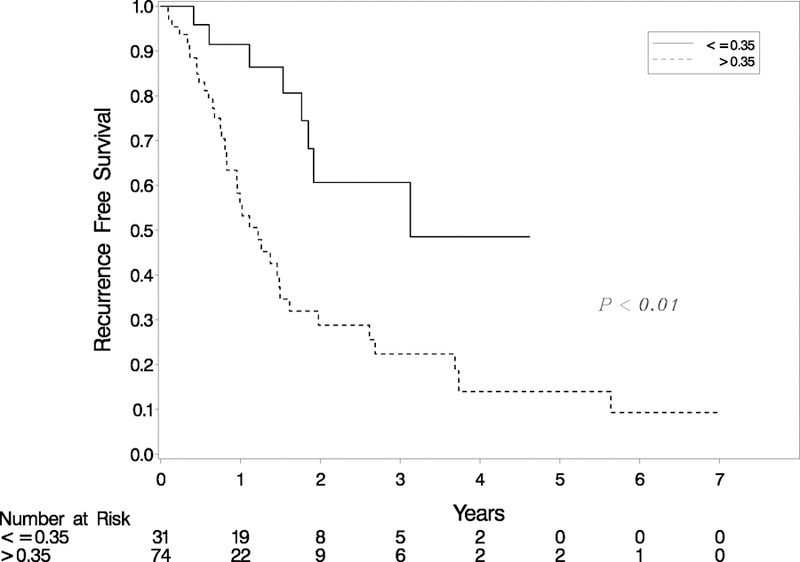
In the setting of neoadjuvant therapy (NAT) for pancreatic ductual adenocarcinoma (PDAC), accurate measurement of tumor size, and consequently, staging based on AJCC eighth edition, is difficult. Attempts to address the limitations of tumor size in the NAT setting have included correlation of residual tumor percent with survival. However, only cases with complete pathologic response or minimal residual disease have shown better prognosis compared with all other groups. To date, no studies have simultaneously evaluated the prognostic value of tumor size and tumor regression in the setting of PDAC status post NAT (NAT-PDAC). Our aim was to study the prognostic value of residual tumor index (RTI), a metric combining residual tumor percent and tumor bed size as an interaction term (% residual tumor×tumor bed size [cm]). In a cohort of 105 cases of NAT-PDAC, we show that RTI supersedes the prognostic value of AJCC eighth edition T staging via multivariate cox regression. At a binary cutoff of 0.35 for RTI, the hazard ratio for recurrence-free survival is 3.26 (95% confidence interval, 1.51-7.04), P<0.01. We further identified cutoffs of ≤0.2, 0.2 to 2 and >2 that stratified our cases into 3 groups via RTI, which were statistically significant in Kaplan-Meier curve analysis of recurrence-free survival (P<0.01) and overall survival (P<0.01). RTI represents a novel metric for combining the prognostic value of tumor size and residual tumor in NAT-PDAC.
在新辅助治疗(NAT)治疗胰腺导管腺癌(PDAC)的情况下,准确测量肿瘤大小,因此,根据 AJCC 第八版进行分期较为困难。为了解决 NAT 环境中肿瘤大小的局限性,人们尝试将残余肿瘤百分比与生存相关联。然而,只有完全病理缓解或最小残留疾病的病例与所有其他组相比显示出更好的预后。迄今为止,尚无研究同时评估 PDAC 状态下 NAT 后(NAT-PDAC)肿瘤大小和肿瘤消退的预后价值。我们的目的是研究残余肿瘤指数(RTI)的预后价值,这是一个结合残余肿瘤百分比和肿瘤床大小的指标,作为交互项(%残余肿瘤×肿瘤床大小[cm])。在 105 例 NAT-PDAC 病例队列中,我们通过多变量 Cox 回归显示,RTI 超过了 AJCC 第八版 T 分期的预后价值。在 RTI 的二进制截止值为 0.35 的情况下,无复发生存的风险比为 3.26(95%置信区间,1.51-7.04),P<0.01。我们进一步确定了 RTI 的≤0.2、0.2 至 2 和>2 的截止值,通过 RTI 将我们的病例分为 3 组,在无复发生存(P<0.01)和总生存(P<0.01)的 Kaplan-Meier 曲线分析中具有统计学意义。RTI 代表了一种新的指标,用于结合 NAT-PDAC 中肿瘤大小和残余肿瘤的预后价值。