Ugawa Ryo, Takigawa Tomoyuki, Shimomiya Hiroko, Ohnishi Takuma, Kurokawa Yuri, Oda Yoshiaki, Shiozaki Yasuyuki, Misawa Haruo, Tanaka Masato, Ozaki Toshifumi
Department of Orthopedic Surgery, Okayama University Hospital, 2-5-1 Shikata-cho, Okayama City, Okayama, 700-8558, Japan.
Division of Medical Support, Okayama University Hospital, 2-5-1 Shikata-cho, Okayama City, Okayama, 700-8558, Japan.
J Orthop Surg Res. 2018 Sep 5;13(1):227. doi: 10.1186/s13018-018-0934-7.
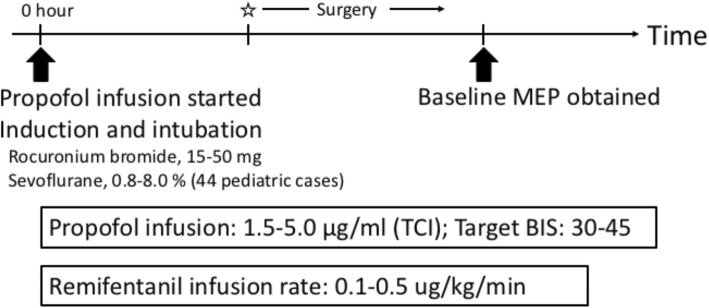
Intraoperative neuromonitoring using motor evoked potentials (MEP) satisfactorily detects motor tract integrity changes during spinal surgery. However, monitoring is affected by "anesthetic fade," in which the stimulation threshold increases because the waveform amplitude decreases with the accumulation of propofol. Therefore, the purpose of this study was to clarify the effect of anesthetic fade on transcranial MEPs by investigating the time-dependent changes of amplitude during spinal deformity surgeries.
We retrospectively reviewed medical records of 142 spinal deformity patients (66 patients with idiopathic scoliosis, 28 with adult spinal deformities, 19 with neuromuscular scoliosis, 17 with syndromic scoliosis, and 12 with congenital scoliosis). The average age was 28 years (range, 5 to 81 years). MEPs were recorded bilaterally from the abductor digiti minimi (ADM) and abductor hallucis (AH) muscles during spinal deformity surgeries. The Wilcoxon signed-rank test was used to investigate the time-dependent changes of amplitude after propofol infusion to evaluate anesthetic fade effects.
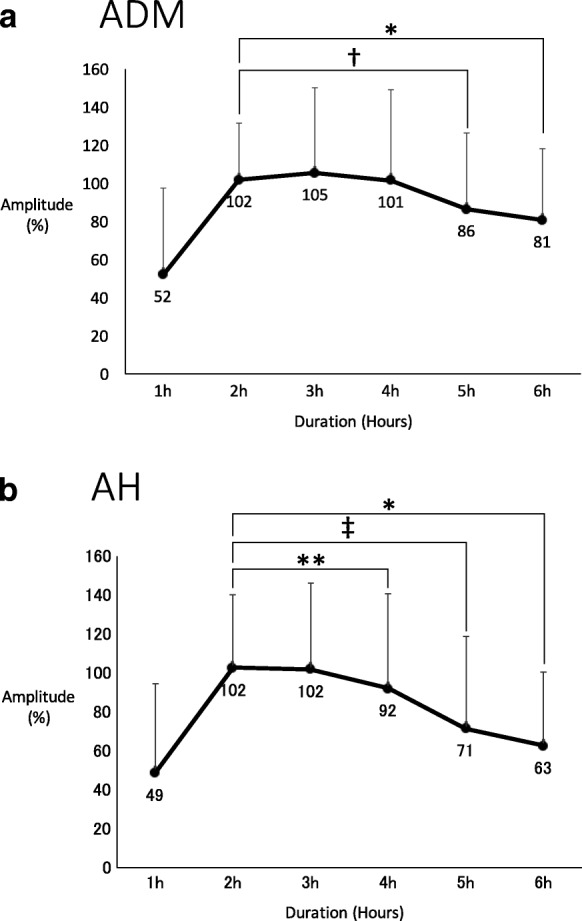
The average time to baseline from initial propofol infusion was 113 min (range, 45 to 182 min). In the ADM, the amplitude was 52% at 1 h after initial propofol infusion, 102% at 2 h, 105% at 3 h, 101% at 4 h, 86% at 5 h, and 81% at 6 h. Compared to the 2-h time point, MEP decreased significantly by 16% at 5 h (P < 0.0005) and by 21% at 6 h (P < 0.05). In the AH, the amplitude was 49% at 1 h after initial infusion of propofol, 102% at 2 h, 102% at 3 h, 92% at 4 h, 71% at 5 h, and 63% at 6 h. Compared to the 2-h time point, MEP decreased significantly by 10% at 4 h (P < 0.005), by 31% at 5 h (P < 0.0000005), and by 39% at 6 h (P < 0.05).
MEP amplitude significantly decreased in the upper limbs at 5 and 6 h and in the lower limbs at 4, 5, and 6 h after the initial infusion of propofol, respectively. The influence of anesthetic fade could influence false positive MEPs during long spinal surgeries.
在脊柱手术中,使用运动诱发电位(MEP)进行术中神经监测能够令人满意地检测运动束完整性的变化。然而,监测会受到“麻醉消退”的影响,即随着丙泊酚的蓄积,刺激阈值会因波形幅度降低而升高。因此,本研究的目的是通过研究脊柱畸形手术期间幅度随时间的变化,阐明麻醉消退对经颅MEP的影响。
我们回顾性分析了142例脊柱畸形患者的病历(66例特发性脊柱侧凸患者、28例成人脊柱畸形患者、19例神经肌肉型脊柱侧凸患者、17例综合征型脊柱侧凸患者和12例先天性脊柱侧凸患者)。平均年龄为28岁(范围为5至81岁)。在脊柱畸形手术期间,从双侧小指展肌(ADM)和拇短展肌(AH)记录MEP。采用Wilcoxon符号秩检验来研究丙泊酚输注后幅度随时间的变化,以评估麻醉消退的影响。
从初始丙泊酚输注到基线的平均时间为113分钟(范围为45至182分钟)。在ADM中,初始丙泊酚输注后1小时幅度为52%,2小时为102%,3小时为105%,4小时为101%,5小时为86%,6小时为81%。与2小时时间点相比,MEP在5小时时显著下降16%(P < 0.0005),在6小时时下降21%(P < 0.05)。在AH中,初始输注丙泊酚后1小时幅度为49%,2小时为102%,3小时为102%,4小时为92%,5小时为71%,6小时为63%。与2小时时间点相比,MEP在4小时时显著下降10%(P < 0.005),在5小时时下降31%(P < 0.0000005),在6小时时下降39%(P < 0.05)。
初始输注丙泊酚后,上肢MEP幅度在5小时和6小时显著下降,下肢MEP幅度在4小时、5小时和6小时分别显著下降。麻醉消退的影响可能会在长时间脊柱手术期间影响MEP假阳性结果。