Shimada Hiroyuki, Doi Takehiko, Lee Sangyoon, Makizako Hyuma, Chen Liang-Kung, Arai Hidenori
Department of Preventive Gerontology, Center for Gerontology and Social Science, National Center for Geriatrics and Gerontology, Obu 474-8511, Japan.
School of Health Sciences, Faculty of Medicine, Kagoshima University, Kagoshima 890-8544, Japan.
J Clin Med. 2018 Aug 30;7(9):250. doi: 10.3390/jcm7090250.
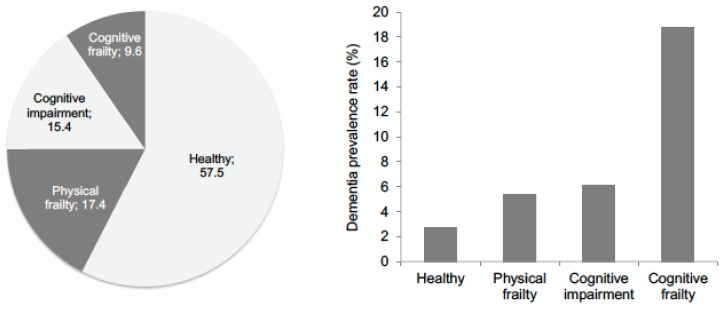
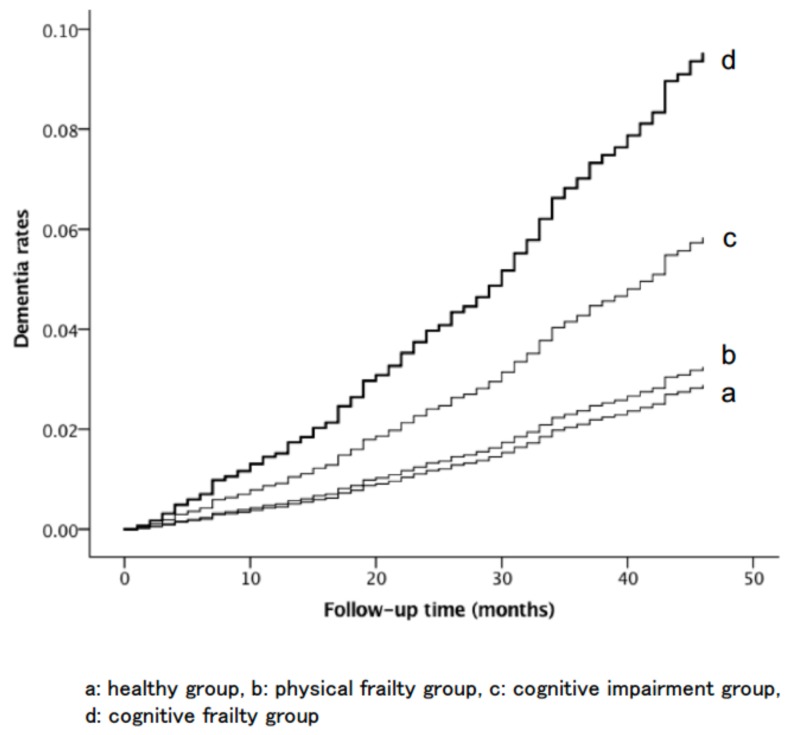
Cognitive frailty, defined as the presence of both frailty and cognitive impairment, is a risk factor for adverse events in older adults. However, prevalence rates of cognitive frailty are low (1.1⁻2.5%), so primary screening is unsuitable in community settings. The aim of the study was to examine whether a new definition of cognitive frailty, which was developed for primary screening, is useful to predict incident dementia in community-dwelling older adults. A total of 4570 older adults participated in the study (2326 women; average age, 71.9 ± 5.5 years). We defined physical frailty as the presence of ≥1 of the following symptoms: slow walking speed and muscle weakness. Cognitive impairment was defined as ≥1 symptom of cognitive impairment, indicated by an age- and education-adjusted score that was ≥1.5 standard deviations below the reference threshold in word list memory, attention, executive function, and processing speed tests. Cognitive frailty was defined as comorbid physical frailty and cognitive impairment. The incidence of dementia was determined using data collected by the Japanese Health Insurance System over 36 months. The prevalence rates of physical frailty, cognitive impairment, and cognitive frailty were 17.5%, 15.3%, and 9.8%, respectively. Cognitive impairment (hazard ratio [HR]: 2.06, 95% confidence interval [95% CI]: 1.41⁻3.02) and cognitive frailty (HR: 3.43, 95% CI: 2.37⁻4.97) were found to be significant risk factors for dementia. However, the association between dementia and physical frailty was not significant (HR: 1.13, 95% CI: 0.76⁻1.69). Individuals with comorbid physical frailty and cognitive impairment could have a higher risk of dementia than healthy older adults or older adults with either physical frailty or cognitive impairment alone.
认知衰弱被定义为同时存在衰弱和认知障碍,是老年人发生不良事件的一个风险因素。然而,认知衰弱的患病率较低(1.1%-2.5%),因此在社区环境中进行初步筛查并不合适。本研究的目的是检验为初步筛查而制定的认知衰弱新定义是否有助于预测社区居住老年人发生痴呆症的情况。共有4570名老年人参与了该研究(2326名女性;平均年龄71.9±5.5岁)。我们将身体衰弱定义为存在以下至少一种症状:步行速度缓慢和肌肉无力。认知障碍被定义为存在至少一种认知障碍症状,通过年龄和教育调整后的分数来表示,该分数在单词列表记忆、注意力、执行功能和处理速度测试中比参考阈值低1.5个标准差以上。认知衰弱被定义为身体衰弱和认知障碍并存。痴呆症的发病率是使用日本医疗保险系统在36个月内收集的数据确定的。身体衰弱、认知障碍和认知衰弱的患病率分别为17.5%、15.3%和9.8%。发现认知障碍(风险比[HR]:2.06,95%置信区间[95%CI]:1.41-3.02)和认知衰弱(HR:3.43,95%CI:2.37-4.97)是痴呆症的重要风险因素。然而,痴呆症与身体衰弱之间的关联并不显著(HR:1.13,95%CI:0.76-1.69)。身体衰弱和认知障碍并存的个体发生痴呆症的风险可能比健康老年人或仅患有身体衰弱或认知障碍的老年人更高。