Department of Cardiothoracic Anaesthesiology, University Hospital of Copenhagen, Rigshospitalet, Blegdamsvej 9, 2100, Copenhagen, Denmark.
Scand J Trauma Resusc Emerg Med. 2018 Sep 10;26(1):75. doi: 10.1186/s13049-018-0537-7.
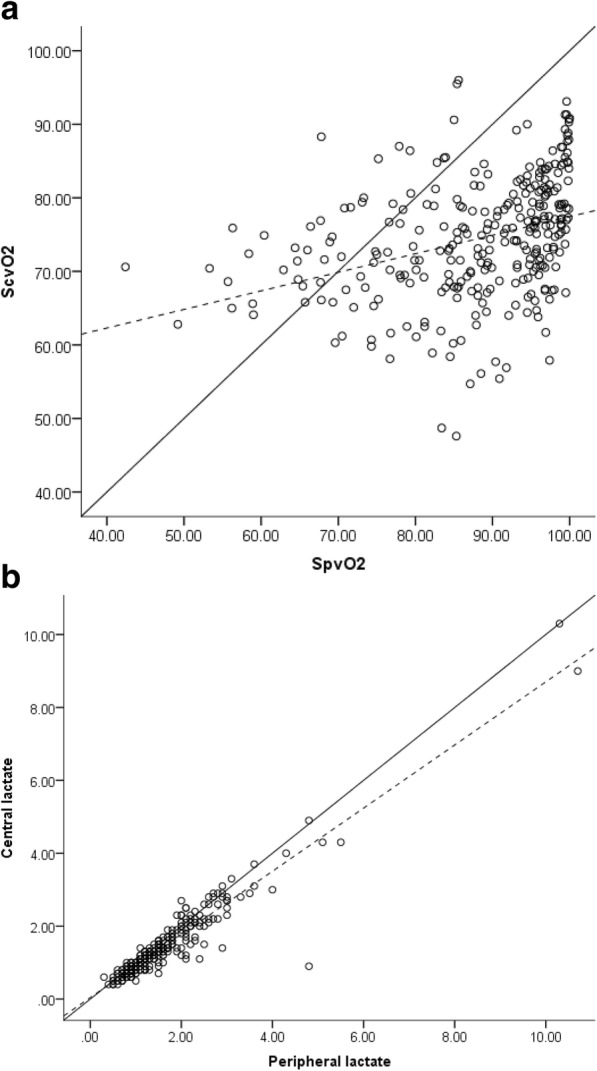
Peripheral measurement of venous oxygen saturation and lactate is a less invasive alternative to monitor tissue oxygenation as compared to measurements from a central venous catheter. However, there is a lack of evidence to support the use of peripheral measurements. In this study, we investigated the agreement between central and peripheral venous oxygen saturation and lactate.
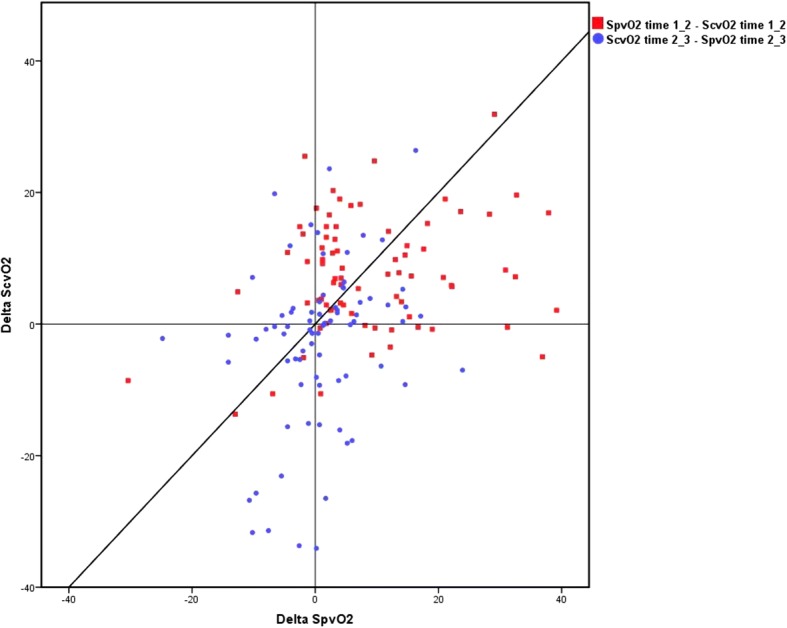
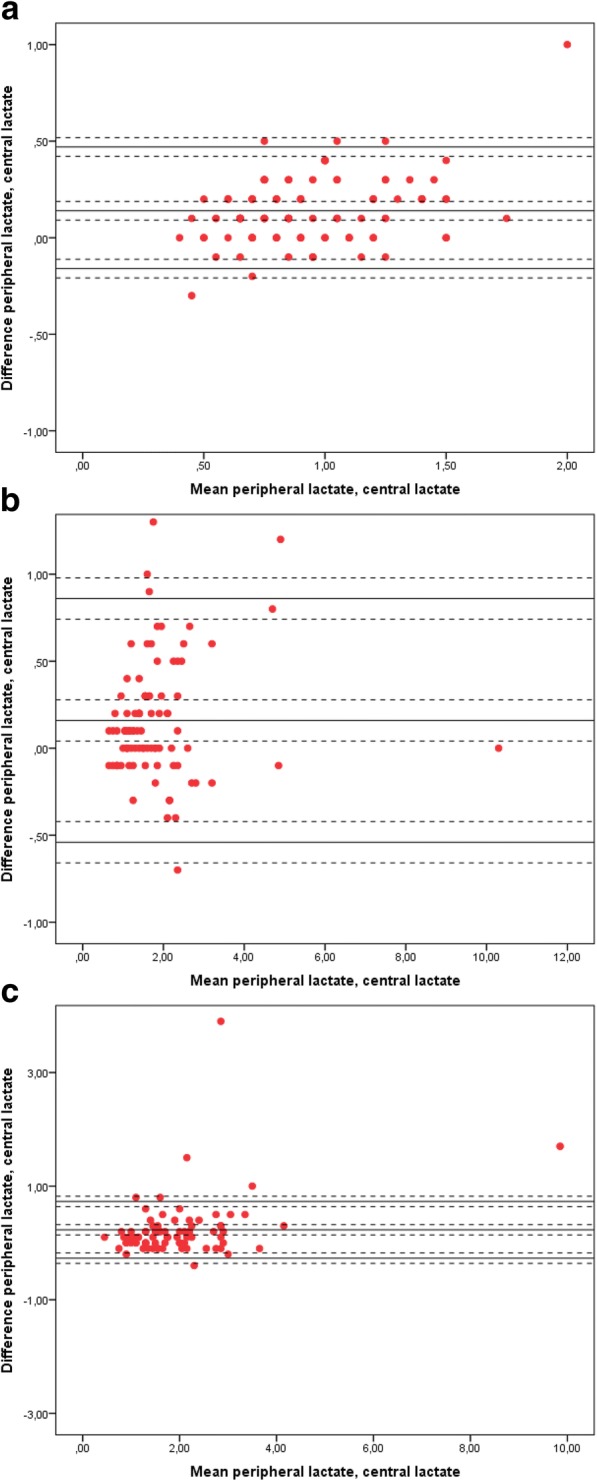
We conducted a prospective observational study including 115 patients who underwent elective cardiac surgery between April and May 2015 at Rigshospitalet, Copenhagen, Denmark. Measurements were obtained simultaneously at induction of anaesthesia, upon arrival in the ICU and 3-4 h postoperatively. Bias and trending ability was identified using Bland-Altman analysis and a four-quadrant plot.
Bias was 13.37% for venous oxygen saturation preoperatively (95% CI: 11.52-15.22, LoA: ±19.10, PE: 22.08%), 11.29% at arrival to the ICU (95% CI: 8.81-13.77, LoA: ±25.10, PE: 32.39%) and 16.49% at 3-4 h postoperatively (95% CI: 14.16-18.82, LoA: ±21.20, PE: 26.82%). A four-quadrant plot demonstrated an 89% concordance. Central and peripheral lactate showed a bias of 0.14 mmol/L preoperatively (95% CI: 0.11-0.17, LoA: ±0.30, PE: 32.08%), 0.16 mmol/L at arrival to ICU (95% CI: 0.09-0.23, LoA: ±0.70, PE: 38.88%) and 0.23 mmol/L at 3-4 h postoperatively (95% CI: 0.11-0.35, LoA: ±0.50, 25.18%).
Measurements of peripheral oxygen saturation and lactate may be valuable in an emergency setting, avoiding unnecessary and time consuming application of a CVC.
We found a high bias but an acceptable trending ability between central and peripheral venous oxygenation. Central and peripheral lactate had excellent agreement. Further studies are necessary to validate the use of peripheral venous samples to identify patients at risk of impaired tissue oxygenation.
与中心静脉导管相比,外周静脉血氧饱和度和乳酸盐的测量是监测组织氧合的一种侵入性较小的替代方法。然而,目前还没有证据支持使用外周测量。在这项研究中,我们调查了中心静脉和外周静脉血氧饱和度和乳酸盐之间的一致性。
我们进行了一项前瞻性观察研究,包括 2015 年 4 月至 5 月在丹麦哥本哈根的 Rigshospitalet 接受择期心脏手术的 115 名患者。在麻醉诱导时、到达 ICU 时和术后 3-4 小时同时进行测量。使用 Bland-Altman 分析和四象限图确定偏倚和趋势能力。
术前静脉血氧饱和度的偏倚为 13.37%(95%CI:11.52-15.22,LoA:±19.10,PE:22.08%),到达 ICU 时为 11.29%(95%CI:8.81-13.77,LoA:±25.10,PE:32.39%),术后 3-4 小时为 16.49%(95%CI:14.16-18.82,LoA:±21.20,PE:26.82%)。四象限图显示 89%的一致性。中心和外周血乳酸盐的术前偏倚为 0.14mmol/L(95%CI:0.11-0.17,LoA:±0.30,PE:32.08%),到达 ICU 时为 0.16mmol/L(95%CI:0.09-0.23,LoA:±0.70,PE:38.88%),术后 3-4 小时为 0.23mmol/L(95%CI:0.11-0.35,LoA:±0.50,PE:25.18%)。
外周血氧饱和度和乳酸盐的测量在紧急情况下可能具有价值,可避免不必要和耗时的中心静脉导管应用。
我们发现中心静脉和外周静脉氧合之间存在较高的偏倚,但具有可接受的趋势能力。中心和外周血乳酸盐具有极好的一致性。需要进一步的研究来验证使用外周静脉样本来识别组织氧合受损的患者。