Vargas Carlos E, Schmidt Matthew Q, Niska Joshua R, Hartsell William F, Keole Sameer R, Doh Lucius, Chang John Han-Chih, Sinesi Christopher, Rodriquez Rossio, Pankuch Mark, Larson Gary L
Department of Radiation Oncology, Mayo Clinic Hospital, Phoenix, Arizona.
Creighton University School of Medicine, Phoenix, Arizona.
Adv Radiat Oncol. 2018 Feb 23;3(3):322-330. doi: 10.1016/j.adro.2018.02.004. eCollection 2018 Jul-Sep.
Randomized evidence for extreme hypofractionation in prostate cancer is lacking. We aimed to identify differences in toxicity and quality-of-life outcomes between standard fractionation and extreme hypofractionated radiation in a phase 3 randomized trial.
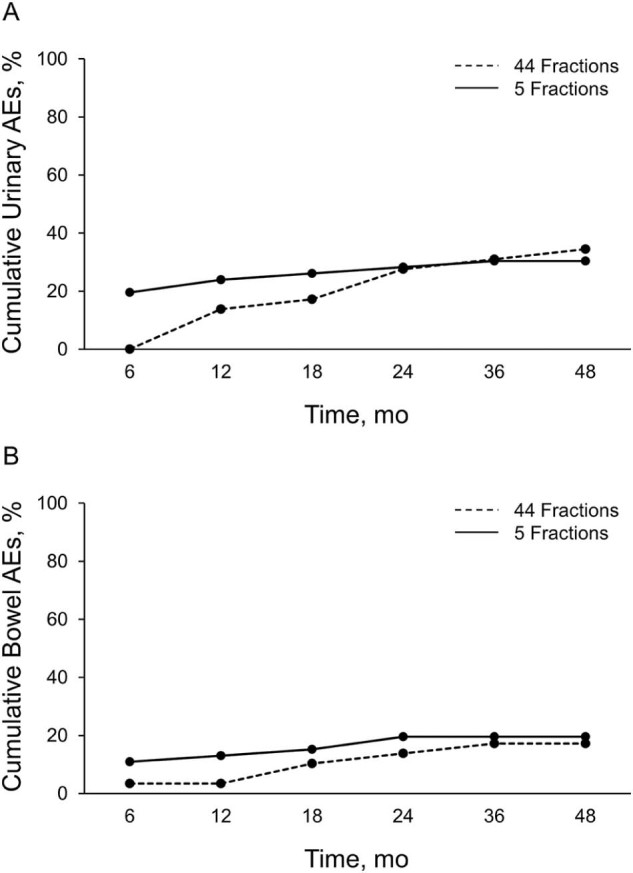
We analyzed the results of the first 75 patients in our phase 3 trial, comparing 38 Gy relative biologic effectiveness (RBE) in 5 fractions (n = 46) versus 79.2 Gy RBE in 44 fractions (n = 29). Patients received proton radiation using fiducials and daily image guidance. We evaluated American Urological Association Symptom Index (AUASI), adverse events (AEs), and Expanded Prostate Index Composite (EPIC) domains. The primary endpoint of this interim analysis was the cumulative incidence of grade 2 (G2) or higher AEs. The randomized patient allocation scheme was a 2:1 ratio favoring the 38 Gy RBE arm.
The median follow-up was 36 months; 30% of patients reached 48-month follow-up. AUASI scores differed <5 points (4.4 vs 8.6; = .002) at 1 year, favoring the 79.2 Gy arm. Differences in AUASI were not significant at ≥18 months. EPIC urinary symptoms favored the 79.2 Gy arm at 1 year (92.3 vs 84.5; = .009) and 18 months (92.3 vs 85.3; = .03); bother scores were not significant at other time points. Cumulative ≥G2 genitourinary toxicity was similar between the 79.2 Gy and 38 Gy arms (34.5% vs 30.4%; = .80). We found no differences in the EPIC domains of bowel symptoms, sexual symptoms, or bowel ≥G2 toxicities. Bladder V80 (79.2 Gy arm; = .04) and V39 (38 Gy arm; = .05) were predictive for cumulative G2 genitourinary AEs.
Low AE rates were seen in both study arms. Early temporary differences in genitourinary scores disappeared over time. Bladder constraints were associated with genitourinary AEs.
前列腺癌超分割放疗的随机证据不足。我们旨在通过一项3期随机试验,确定标准分割放疗与超分割放疗在毒性和生活质量结果方面的差异。
我们分析了3期试验中前75例患者的结果,比较了5次分割照射38 Gy相对生物效应(RBE)(n = 46)与44次分割照射79.2 Gy RBE(n = 29)的情况。患者使用基准标记和每日图像引导接受质子放疗。我们评估了美国泌尿外科学会症状指数(AUASI)、不良事件(AE)和扩展前列腺指数综合评分(EPIC)各领域。本次中期分析的主要终点是2级(G2)或更高等级AE的累积发生率。随机患者分配方案为2:1,倾向于38 Gy RBE组。
中位随访时间为36个月;30%的患者达到48个月随访。1年时,AUASI评分差异<5分(4.4对8.6;P = 0.002),79.2 Gy组更优。≥18个月时,AUASI差异无统计学意义。1年时(92.3对84.5;P = 0.009)和18个月时(92.3对85.3;P = 0.03),EPIC泌尿系统症状79.2 Gy组更优;其他时间点的困扰评分无统计学意义。79.2 Gy组和38 Gy组累积≥G2级泌尿生殖系统毒性相似(34.5%对30.4%;P = 0.80)。我们发现肠道症状、性功能症状的EPIC各领域或肠道≥G2级毒性无差异。膀胱V80(79.2 Gy组;P = 0.04)和V39(38 Gy组;P = 0.05)可预测累积G2级泌尿生殖系统AE。
两个研究组的AE发生率均较低。泌尿生殖系统评分的早期暂时差异随时间消失。膀胱限制与泌尿生殖系统AE相关。