Department of Radiation Oncology, Mayo Clinic, Rochester, Minnesota.
Department of Immunology, Mayo Clinic, Rochester, Minnesota.
Int J Radiat Oncol Biol Phys. 2019 Jan 1;103(1):229-240. doi: 10.1016/j.ijrobp.2018.09.001. Epub 2018 Sep 8.
This study examined the effects of metastasis-directed stereotactic body radiation therapy (mdSBRT) on CD8 T-cell subpopulations and correlated post-mdSBRT immunophenotypic responses with clinical outcomes in patients with oligometastatic prostate cancer (OPCa).
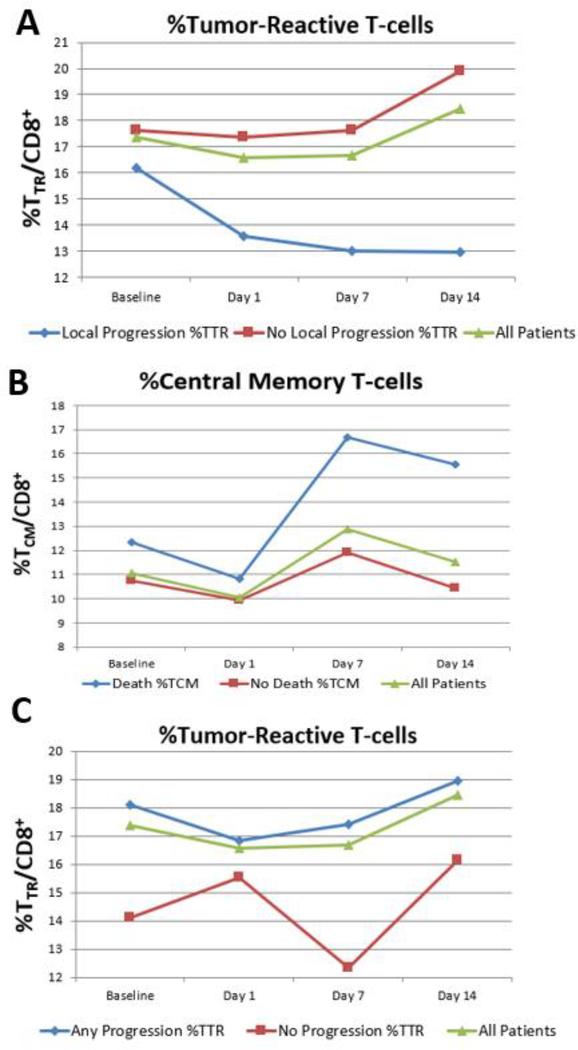
Peripheral blood mononuclear cells were prospectively isolated from 37 patients with OPCa (≤3 metastases) who were treated with mdSBRT. Immunophenotyping identified circulating CD8 T-cell subpopulations, including tumor-reactive (T), effector memory, central memory (T), effector, and naïve T cells from samples collected before and after mdSBRT. Univariate Cox proportional hazards regression was used to assess whether changes in these T-cell subpopulations were potential risk factors for death and/or progression. The Kaplan-Meier method was used for survival. Cumulative incidence for progression and new distant metastasis weas estimated, considering death as a competing risk.
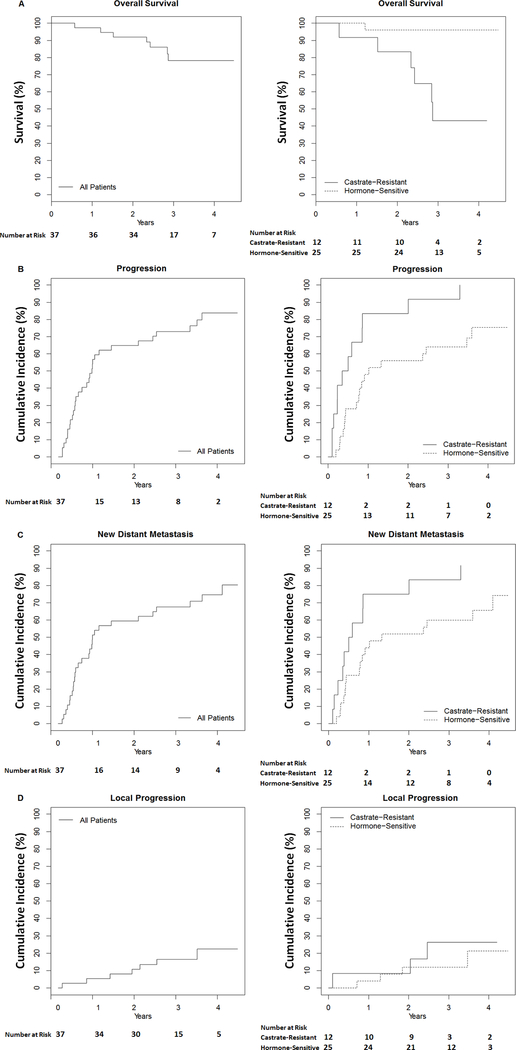
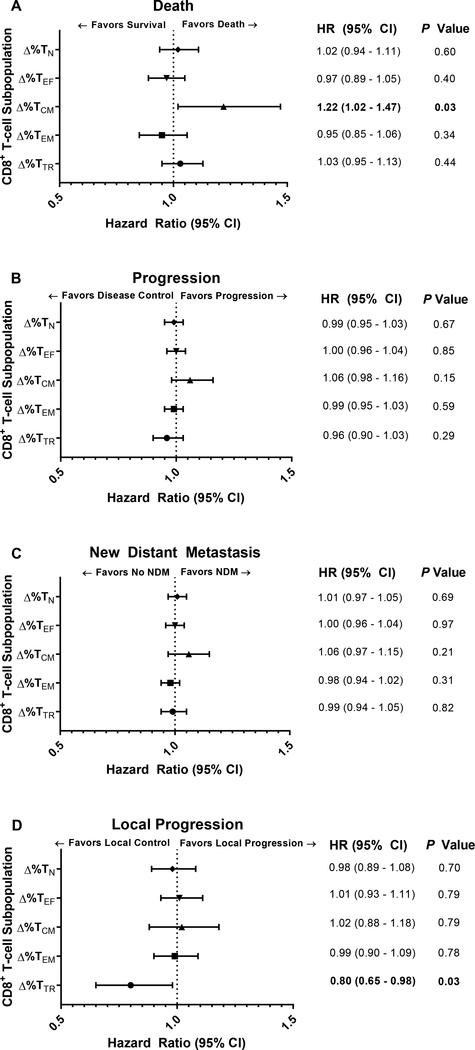
Median follow-up was 39 months (interquartile range, 34-43). Overall survival at 3 years was 78.2%. Cumulative incidence for local progression and new distant metastasis at 3 years was 16.5% and 67.6%, respectively. Between baseline and day 14 after mdSBRT, an increase in the T cell subpopulation was associated with the risk of death (hazard ratio, 1.22 [95% confidence interval, 1.02-1.47]; P = .033), and an increase in the T cell subpopulation was protective against the risk of local progression (hazard ratio, 0.80 [95% confidence interval, 0.65-0.98]; P = .032).
An increase in the T cell subpopulation was protective against the risk of disease progression, and an increase in the T cell subpopulation was associated with the risk of death in patients with OPCa treated with mdSBRT. Disease control may be further improved by better understanding the CD8 T-cell subpopulations and by enhancing their antitumor effect.
本研究旨在探讨转移性定向立体定向放疗(mdSBRT)对寡转移性前列腺癌(OPCa)患者 CD8 T 细胞亚群的影响,并将 post-mdSBRT 免疫表型反应与临床结果相关联。
前瞻性地从 37 例接受 mdSBRT 治疗的 OPCa(≤3 个转移灶)患者中分离外周血单核细胞。免疫表型分析鉴定循环 CD8 T 细胞亚群,包括治疗前和治疗后采集的样本中的肿瘤反应性(T)、效应记忆、中央记忆(T)、效应和幼稚 T 细胞。单变量 Cox 比例风险回归用于评估这些 T 细胞亚群的变化是否为死亡和/或进展的潜在危险因素。Kaplan-Meier 法用于生存分析。考虑死亡为竞争风险,使用累积发生率来估计进展和新发远处转移的情况。
中位随访时间为 39 个月(四分位距,34-43)。3 年总生存率为 78.2%。3 年时局部进展和新发远处转移的累积发生率分别为 16.5%和 67.6%。在 mdSBRT 前后第 14 天,T 细胞亚群增加与死亡风险相关(风险比,1.22[95%置信区间,1.02-1.47];P=0.033),T 细胞亚群增加可降低局部进展风险(风险比,0.80[95%置信区间,0.65-0.98];P=0.032)。
T 细胞亚群增加可降低 OPCa 患者接受 mdSBRT 治疗后疾病进展的风险,T 细胞亚群增加与死亡风险相关。通过更好地了解 CD8 T 细胞亚群并增强其抗肿瘤作用,可能进一步改善疾病控制。