Division of General Internal Medicine, University of California San Francisco, San Francisco, CA 94123, USA.
Division of Hospital Medicine, University of California San Francisco, San Francisco, CA, USA.
BMJ. 2018 Sep 12;362:k3503. doi: 10.1136/bmj.k3503.
To assess how often older adults admitted to hospital for common non-cardiac conditions were discharged with intensified antihypertensive treatment, and to identify markers of appropriateness for these intensifications.
Retrospective cohort study.
US Veterans Administration Health System.
Patients aged 65 years or over with hypertension admitted to hospital with non-cardiac conditions between 2011 and 2013.
Intensification of antihypertensive treatment, defined as receiving a new or higher dose antihypertensive agent at discharge compared with drugs used before admission. Hierarchical logistic regression analyses were used to control for characteristics of patients and hospitals.
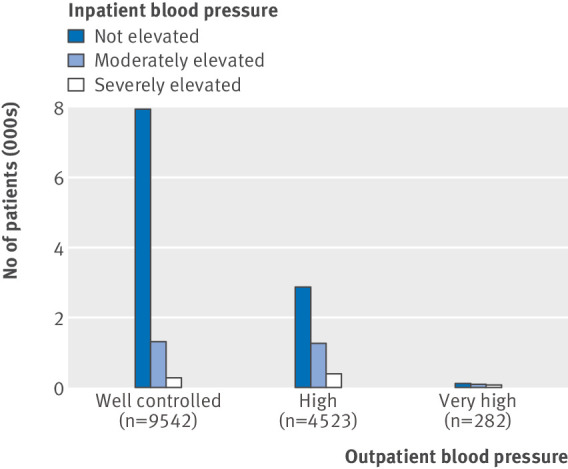
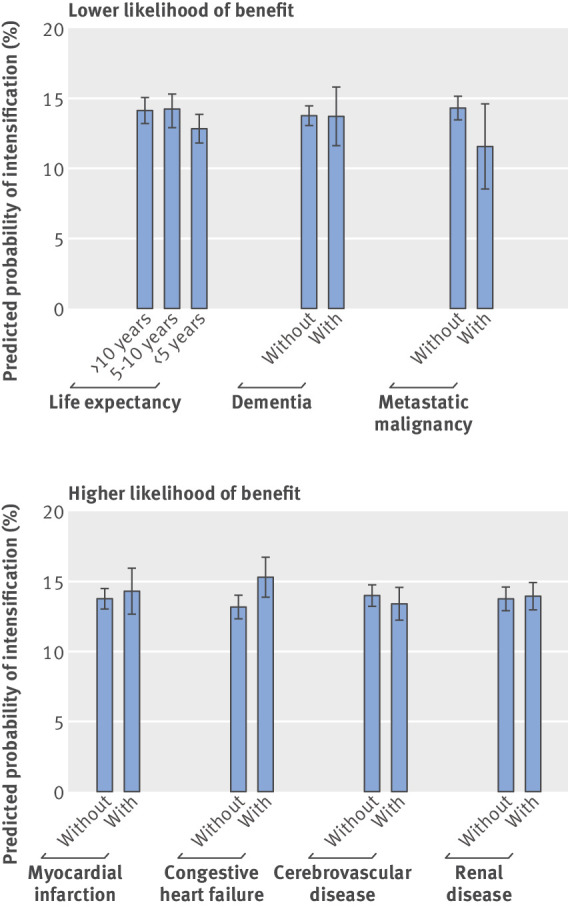
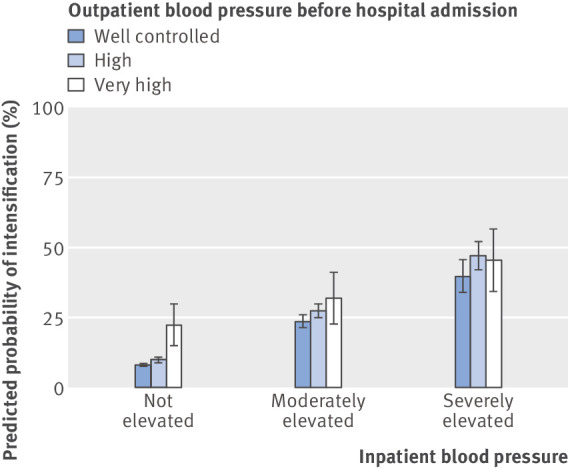
Among 14 915 older adults (median age 76, interquartile range 69-84), 9636 (65%) had well controlled outpatient blood pressure before hospital admission. Overall, 2074 (14%) patients were discharged with intensified antihypertensive treatment, more than half of whom (1082) had well controlled blood pressure before admission. After adjustment for potential confounders, elevated inpatient blood pressure was strongly associated with being discharged on intensified antihypertensive regimens. Among patients with previously well controlled outpatient blood pressure, 8% (95% confidence interval 7% to 9%) of patients without elevated inpatient blood pressure, 24% (21% to 26%) of patients with moderately elevated inpatient blood pressure, and 40% (34% to 46%) of patients with severely elevated inpatient blood pressure were discharged with intensified antihypertensive regimens. No differences were seen in rates of intensification among patients least likely to benefit from tight blood pressure control (limited life expectancy, dementia, or metastatic malignancy), nor in those most likely to benefit (history of myocardial infarction, cerebrovascular disease, or renal disease).
One in seven older adults admitted to hospital for common non-cardiac conditions were discharged with intensified antihypertensive treatment. More than half of intensifications occurred in patients with previously well controlled outpatient blood pressure. More attention is needed to reduce potentially harmful overtreatment of blood pressure as older adults transition from hospital to home.
评估因常见非心脏疾病住院的老年患者出院时强化降压治疗的频率,并确定这些强化治疗的适宜性指标。
回顾性队列研究。
美国退伍军人事务部医疗系统。
2011 年至 2013 年间患有高血压并因非心脏疾病住院的 65 岁及以上患者。
降压治疗的强化,定义为与入院前使用的药物相比,出院时接受新的或更高剂量的降压药物。采用分层逻辑回归分析来控制患者和医院的特征。
在 14915 名老年患者中(中位年龄 76 岁,四分位间距 69-84),9636 名(65%)患者在入院前门诊血压控制良好。总体而言,2074 名(14%)患者出院时接受了强化降压治疗,其中一半以上(1082 名)患者在入院前血压控制良好。在校正潜在混杂因素后,住院期间血压升高与出院时接受强化降压方案密切相关。在门诊血压控制良好的患者中,无升高的住院期间血压的患者中有 8%(95%置信区间 7%-9%)、中度升高的住院期间血压的患者中有 24%(21%-26%)、严重升高的住院期间血压的患者中有 40%(34%-46%)出院时接受了强化降压方案。在最不可能从严格血压控制中获益的患者(预期寿命有限、痴呆或转移性恶性肿瘤)和最有可能获益的患者(心肌梗死、脑血管病或肾脏疾病史)中,强化治疗的比例没有差异。
每 7 名因常见非心脏疾病住院的老年患者中就有 1 名出院时接受强化降压治疗。超过一半的强化治疗发生在门诊血压控制良好的患者中。随着老年患者从医院过渡到家庭,需要更加注意减少潜在的有害过度降压治疗。