1Department of Clinical Science, University of Bergen, Bergen, Norway.
2Norwegian Advisory Unit for Antibiotic Use in Hospitals, Department of Research and Development, Haukeland University Hospital, Jonas Lies vei 65, N-5021 Bergen, Norway.
Antimicrob Resist Infect Control. 2018 Sep 10;7:109. doi: 10.1186/s13756-018-0400-7. eCollection 2018.
There is limited evidence from multicenter, randomized controlled studies to inform planning and implementation of antibiotic stewardship interventions in hospitals.
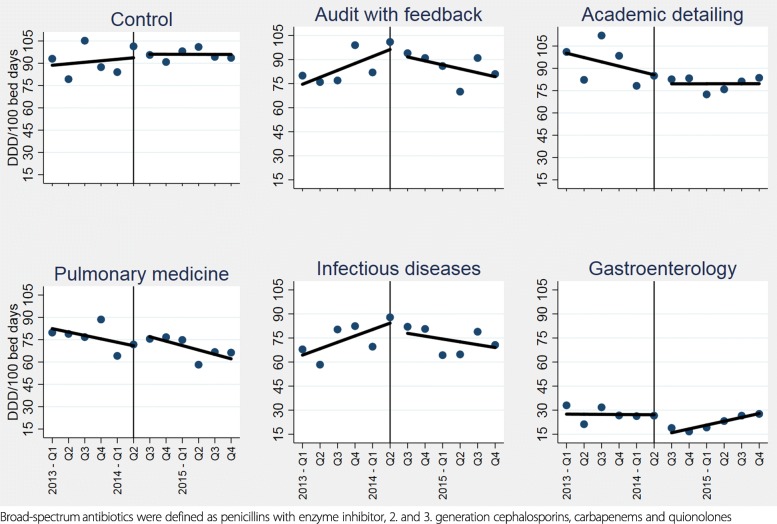
A cluster randomized, controlled, intervention study was performed in selected specialities (infectious diseases, pulmonary medicine and gastroenterology) at three emergency care hospitals in Western Norway. Interventions applied were audit with feedback and academic detailing. Implementation strategies included co-design of interventions with stakeholders in local intervention teams and prescribers setting local targets for change in antibiotic prescribing behaviour. Primary outcome measures were adherence to national guidelines, use of broad-spectrum antibiotics and change in locally defined targets of change in prescribing behaviour. Secondary outcome measures were length of stay, 30-day readmission, in-hospital- and 30-day mortality.
One thousand eight hundred two patients receiving antibiotic treatment were included. Adherence to guidelines had an absolute increase from 60 to 66% for all intervention wards ( = 0.04). Effects differed across specialties and pulmonary intervention wards achieved a 14% absolute increase in adherence ( = 0.003), while no change was observed for other specialties. A pulmonary ward targeting increased use of penicillin G 2 mill IU × 4 for pneumonia and COPD exacerbations had an intended increase of 30% for this prescribing behaviour ( < 0.001).
Pulmonary wards had a higher increase in adherence, independent of applied intervention. The effect of antibiotic stewardship interventions is dependent on how and in which context they are implemented. Additional effects of interventions are seen when stakeholders discuss ward prescribing behaviour and agree on specific targets for changes in prescribing practice.
多中心、随机对照研究提供的证据有限,无法为医院抗生素管理干预措施的规划和实施提供信息。
在挪威西部的三家急诊医院的特定科室(传染病、呼吸医学和胃肠病学)进行了一项集群随机对照干预研究。应用的干预措施是审核和反馈以及学术细化。实施策略包括与当地干预团队的利益相关者共同设计干预措施,以及规定当地改变抗生素处方行为的目标。主要结局指标是遵守国家指南、使用广谱抗生素和改变当地定义的处方行为目标。次要结局指标是住院时间、30 天再入院率、院内和 30 天死亡率。
共纳入 1802 例接受抗生素治疗的患者。所有干预病房的指南遵守率从 60%绝对增加到 66%( = 0.04)。效果因专业而异,呼吸干预病房的遵医嘱率绝对增加了 14%( = 0.003),而其他科室没有变化。针对肺炎和 COPD 加重症增加青霉素 G 2 万 IU×4 使用率的肺部病房,这一用药行为的预期增加了 30%( < 0.001)。
肺部病房的遵医嘱率增加更高,与应用的干预措施无关。抗生素管理干预措施的效果取决于实施方式和实施环境。当利益相关者讨论病房的处方行为并就处方实践的具体目标达成一致时,干预措施会产生额外的效果。