Matsumoto Michinori, Wakiyama Shigeki, Shiba Hiroaki, Haruki Koichiro, Futagawa Yasuro, Ishida Yuichi, Misawa Takeyuki, Yanaga Katsuhiko
Department of Surgery, The Jikei University School of Medicine, Tokyo 105-8461, Japan.
Mol Clin Oncol. 2018 Oct;9(4):369-376. doi: 10.3892/mco.2018.1692. Epub 2018 Aug 6.
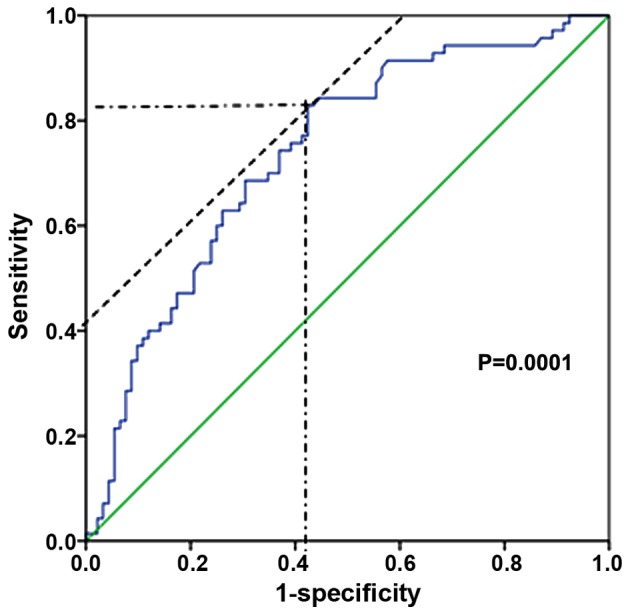
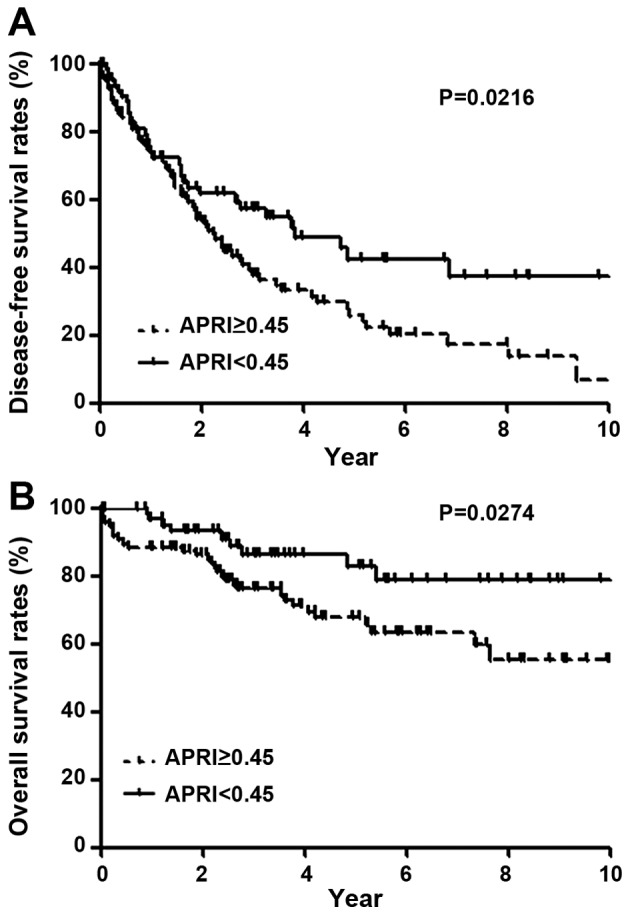
Liver function is a major prognostic factor following hepatic resection for hepatocellular carcinoma (HCC), which is well correlated with the degree of fibrosis. On the other hand, the presence of liver cirrhosis itself leads to a higher incidence of HCC than chronic hepatitis. Therefore, preoperative noninvasive markers of fibrosis are important for the assessment of prognosis for treatment of HCC. The present study aimed to analyze whether aspartate aminotransferase to platelet ratio index (APRI) could predict prognosis following hepatic resection for HCC. The subjects were 162 patients who underwent hepatic resection for HCC between January 2000 and December 2011. The relationship between APRI and disease-free and overall survival were retrospectively investigated. In multivariate analysis, indocyanine green at 15 min (ICG-R15) ≥15% (P=0.0306), APRI ≥0.45 (P=0.0184), perioperative blood transfusion of red cell concentrates (RCC; P=0.0034) and TNM stage II, III or IV (P=0.0184) were significant predictors in disease-free survival. For overall survival, ICG-R15 ≥15% (P=0.0454), APRI ≥0.45 (P=0.0417), perioperative blood transfusion of RCC (P=0.0036) and TNM stage II, III or IV (P=0.0033) were significant predictors. In addition, higher APRI values were positively correlated with hepatitis C virus infection and preoperative liver function. In conclusion, APRI is an independent risk factor for disease-free and overall survival following hepatic resection for HCC.
肝功能是肝细胞癌(HCC)肝切除术后的一个主要预后因素,与纤维化程度密切相关。另一方面,肝硬化本身导致HCC的发病率高于慢性肝炎。因此,术前纤维化的非侵入性标志物对于评估HCC治疗的预后很重要。本研究旨在分析天冬氨酸转氨酶与血小板比值指数(APRI)是否可以预测HCC肝切除术后的预后。研究对象为2000年1月至2011年12月期间接受HCC肝切除术的162例患者。回顾性研究了APRI与无病生存期和总生存期之间的关系。在多变量分析中,15分钟靛氰绿滞留率(ICG-R15)≥15%(P=0.0306)、APRI≥0.45(P=0.0184)、围手术期输注红细胞浓缩液(RCC;P=0.0034)以及TNM分期II、III或IV期(P=0.0184)是无病生存期的显著预测因素。对于总生存期,ICG-R15≥15%(P=0.0454)、APRI≥0.4(P=0.0417)、围手术期输注RCC(P=0.0036)以及TNM分期II、III或IV期(P=0.0033)是显著预测因素。此外,较高的APRI值与丙型肝炎病毒感染和术前肝功能呈正相关。总之,APRI是HCC肝切除术后无病生存期和总生存期的独立危险因素。