Che Xiajing, Yang Xiaoqian, Yan Jiayi, Yuan Yanhong, Ma Qing, Ying Liang, Zhang Minfang, Wang Qin, Zhang Ming, Ni Zhaohui, Mou Shan
Department of Nephrology, Molecular Cell Laboratory for Kidney Disease, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, 160 Pujian Road, Shanghai, 200127, China.
Transplantation Center of Ren Ji Hospital, School of Medicine, Shanghai Jiao Tong University, 160 Pujian Road, Shanghai, 200127, China.
BMC Nephrol. 2018 Sep 17;19(1):235. doi: 10.1186/s12882-018-1013-3.
The effect of pretransplant peritoneal dialysis (PD) or hemodialysis (HD) modality on outcomes of kidney transplantation (KT) for end-stage renal disease (ESRD) is debatable. We evaluated the outcomes these modalities in KT from donor after cardiac death (DCD).
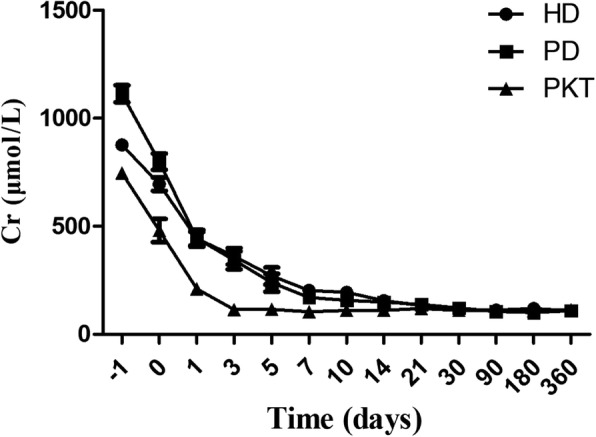
A cohort of 251 patients on HD, PD or pre-emptive who underwent first KT from DCD between January 2014 and December 2016 were prospectively analyzed to compare for outcomes on recovery of renal function, complications as well as patient and graft survival. The patients were followed till August 2017. Data on 104 HD and 98 PD were available for final comparative outcome analysis, 5 pre-emptive were analyzed as the control group.
Both HD and PD group patients were well matched for demographic and baseline characteristics. The follow-up period was 12.5 (3.0, 22.0) months in HD and 12.0 (6.0, 20.0) months in PD patients. Post-transplant renal functions between the two groups showed no differences. Among PD patients, 16 (16.3%) suffered delayed graft function, versus 19 (18.3%) in HD, with no statistical differences (p = 0.715). Complications of acute rejection, infections were comparable between the groups. The patient survival, graft survival and death-censored graft survival were similar for HD and PD after adjusting for other multiple risk factors.
Our results indicate that outcome of first KT from DCD is not affected by pretransplant dialysis modality of PD or HD in aspects of recovery of renal function, complications as well as patient and graft survival.
肾移植前腹膜透析(PD)或血液透析(HD)模式对终末期肾病(ESRD)患者肾移植(KT)结局的影响存在争议。我们评估了这些模式在心脏死亡后供体肾移植(DCD)中的结局。
前瞻性分析了2014年1月至2016年12月期间接受首次DCD肾移植的251例接受HD、PD或抢先肾移植的患者,以比较肾功能恢复、并发症以及患者和移植物存活情况。对患者随访至2017年8月。104例HD患者和98例PD患者的数据可用于最终比较结局分析,5例抢先肾移植患者作为对照组进行分析。
HD组和PD组患者在人口统计学和基线特征方面匹配良好。HD组患者的随访期为12.5(3.0,22.0)个月,PD组患者为12.0(6.0,20.0)个月。两组移植后肾功能无差异。PD患者中,16例(16.3%)发生移植肾功能延迟,HD患者中为19例(18.3%),无统计学差异(p = 0.715)。两组急性排斥反应、感染等并发症相当。在调整其他多种危险因素后,HD组和PD组的患者生存率、移植物生存率和死亡删失移植物生存率相似。
我们的结果表明,在肾功能恢复、并发症以及患者和移植物存活方面,DCD首次肾移植的结局不受移植前PD或HD透析模式的影响。