Department of Orthopaedic Surgery, Hokusuikai Kinen Hospital, 3-2-1 Higashihara, Mito, Ibaraki, 310-0035, Japan.
Department of Anesthesiology, Hokusuikai Kinen Hospital, Mito, Japan.
Knee Surg Sports Traumatol Arthrosc. 2019 Apr;27(4):1124-1131. doi: 10.1007/s00167-018-5140-y. Epub 2018 Sep 20.
This study was performed to determine whether periarticular injection performed in the early stage of total knee arthroplasty (TKA) could provide a better postoperative pain relief than periarticular injection performed in the late stage of TKA. The hypothesis was based on the concept that analgesic intervention before the onset of noxious stimuli would be associated with less postoperative pain.
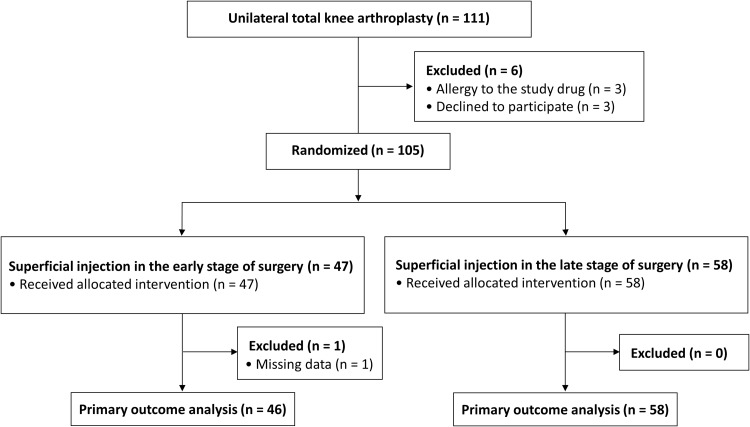
A total of 105 participants were randomly assigned to receive superficial injection just prior to arthrotomy (early stage periarticular injection group) or superficial injection after implanting the prosthesis (late-stage periarticular injection group) in patients undergoing unilateral TKA with 1:1 treatment allocation. In both groups, deep injection was performed according to the same schedule (just prior to implanting prosthesis). The solution consisted of 300 mg of ropivacaine, 8 mg of morphine, 40 mg of methylprednisolone, 50 mg of ketoprofen, and 0.3 mg of epinephrine mixed with normal saline to a final volume of 60 mL. All surgeries were managed under general anesthesia without any regional blocks. Registry-specified primary outcome was postoperative pain score at rest measured at the recovery room using a 100-mm visual analog scale (VAS). The VAS score was compared between two groups and assessed to reach the reported threshold values for the minimal clinically important difference (MCID) of 10 mm for the postoperative VAS score.
The VAS score at the recovery room was significantly lower in the early stage periarticular injection group than the late-stage periarticular injection group (23 ± 25 mm versus 39 ± 34 mm, respectively; 95% confidence interval 4-28 mm; p = 0.0078). The mean difference in the primary outcome fulfilled the MCID value.
Bringing forward the timing of periarticular injection may provide significant and clinically meaningful improvement in pain following TKA under general anesthesia.
I.
本研究旨在确定全膝关节置换术(TKA)早期行关节周围注射是否比 TKA 晚期行关节周围注射能提供更好的术后疼痛缓解。该假设基于这样的概念,即在有害刺激出现之前进行镇痛干预将与术后疼痛减轻相关。
共 105 名患者被随机分配接受单侧 TKA,按 1:1 治疗分配,一组在关节切开前(早期关节周围注射组)接受浅层注射,另一组在植入假体后(晚期关节周围注射组)接受浅层注射。两组均按照相同的方案进行深层注射(在植入假体前)。溶液由 300mg 罗哌卡因、8mg 吗啡、40mg 甲泼尼龙、50mg 酮咯酸和 0.3mg 肾上腺素与生理盐水混合至最终体积 60mL。所有手术均在全身麻醉下进行,不使用任何区域阻滞。注册指定的主要结局是在恢复室使用 100mm 视觉模拟量表(VAS)测量的静息时术后疼痛评分。比较两组之间的 VAS 评分,并评估是否达到术后 VAS 评分最小临床重要差异(MCID)10mm 的报告阈值。
早期关节周围注射组在恢复室的 VAS 评分明显低于晚期关节周围注射组(分别为 23±25mm 与 39±34mm;95%置信区间 4-28mm;p=0.0078)。主要结局的平均差异符合 MCID 值。
在全身麻醉下进行 TKA 时,提前进行关节周围注射可能会显著改善术后疼痛,并具有临床意义。
I。