Department of Clinical Sciences, Ophthalmology, Umeå University, Umeå, Sweden.
Department of Clinical Sciences in Malmö, Ophthalmology, Lund University, Malmö, Sweden.
Acta Ophthalmol. 2018 Sep;96(6):567-572. doi: 10.1111/aos.13790. Epub 2018 Sep 21.
To study newly diagnosed glaucoma patients given mono- or multi-therapy regarding differences in initial intraocular pressure (IOP) reduction, target IOP levels reached and influence of untreated baseline IOP on IOP reduction.
Patients newly diagnosed with manifest primary open-angle glaucoma and included in the Glaucoma Intensive Treatment Study (GITS) were randomized to immediate intensive treatment with any of three different IOP-lowering substances supplied in two bottles plus 360° laser trabeculoplasty or to conventional stepwise treatment starting with a single-drug. Intraocular pressure reduction was analysed 1 month after initiation of treatment.
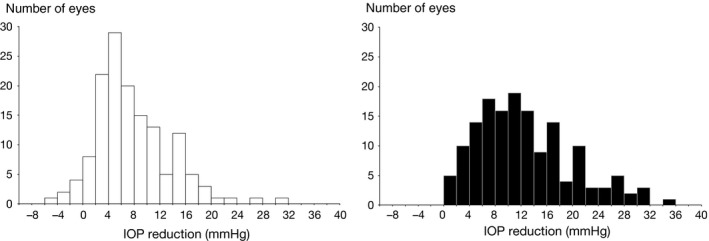
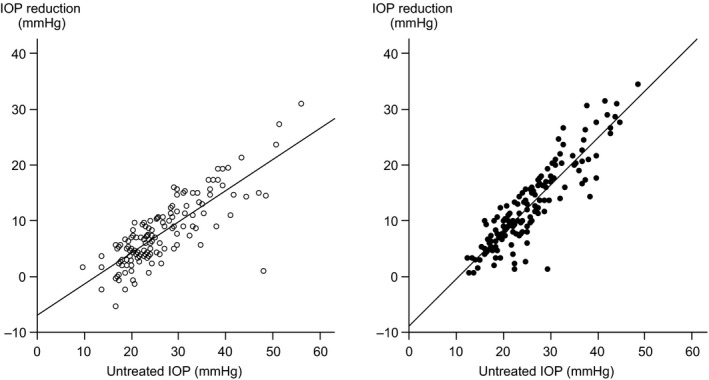
One hundred eighteen patients (143 eyes) received mono-therapy and 122 patients (152 eyes) multi-therapy. Median baseline IOP was 24.0 (min: 9.7, max: 56.0) mmHg in mono-therapy eyes and 24.0 (min: 12.3, max: 48.5) mmHg in multi-therapy eyes (p = 0.56). After 1 month in the two groups, respectively, values for median IOP reduction were 6.3 (range: -5.3-31.0) and 11.0 (range: 0.7-34.5) mmHg, and for mean relative decline 26.8 (range: -32.0-55.4) and 46.0 (range: 4.6-81.6) % (p = 0.000). A larger proportion of the multi-therapy patients reached each target IOP level (p = 0.000). The higher the baseline IOP, the larger the observed pressure reduction, considering both absolute and relative figures. The effect was more pronounced in eyes with multi-therapy than in those with mono-therapy (p = 0.000). For every mmHg higher IOP at baseline, the IOP was reduced by an additional 0.56 (mono-therapy) or 0.84 (multi-therapy) mmHg.
Intensive treatment led to considerably greater IOP reduction than mono-therapy. Among patients with IOP ≥30 mmHg at diagnosis an IOP of <16 was reached in 2/3 of those with multi-therapy but in none with mono-therapy. The IOP reduction was highly dependent on the untreated IOP level.
研究新诊断为青光眼的患者接受单药或多药治疗,观察初始眼压(IOP)降低、目标眼压水平的差异以及未治疗的基线眼压对眼压降低的影响。
将新诊断为显性原发性开角型青光眼的患者纳入青光眼强化治疗研究(GITS),并随机分为两组:立即接受三种不同的降眼压药物联合两种药物的强化治疗(激光小梁成形术),或接受从单一药物开始的常规逐步治疗。在开始治疗后 1 个月分析眼压降低情况。
118 例(143 只眼)患者接受单药治疗,122 例(152 只眼)患者接受多药治疗。单药治疗组的中位基线眼压为 24.0(最小:9.7,最大:56.0)mmHg,多药治疗组为 24.0(最小:12.3,最大:48.5)mmHg(p=0.56)。两组治疗 1 个月后,IOP 中位数分别降低 6.3(范围:-5.3-31.0)mmHg 和 11.0(范围:0.7-34.5)mmHg,平均相对下降分别为 26.8(范围:-32.0-55.4)%和 46.0(范围:4.6-81.6)%(p=0.000)。更多的多药治疗患者达到了每个目标眼压水平(p=0.000)。基线眼压越高,绝对和相对眼压降低值越大。在多药治疗组中,这种效应比单药治疗组更为明显(p=0.000)。对于每增加 1mmHg 的基线眼压,眼压降低 0.56mmHg(单药治疗)或 0.84mmHg(多药治疗)。
强化治疗比单药治疗能显著降低眼压。在诊断时眼压≥30mmHg 的患者中,多药治疗组有 2/3的患者眼压降至<16mmHg,而单药治疗组无一例达到。眼压降低与未治疗的眼压水平高度相关。