Clinical Research Centre, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark.
The Acute Medical Unit, The Emergency Department, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark.
Crit Care Med. 2018 Dec;46(12):1961-1968. doi: 10.1097/CCM.0000000000003441.
Soluble urokinase plasminogen activator receptor is a prognostic biomarker associated with critical illness, disease progression, and risk of mortality. We aimed to evaluate whether soluble urokinase plasminogen activator receptor adds prognostic value to a vital sign-based score for clinical monitoring of patient risk (National Early Warning Score) in acute medical patients.
Registry-based observational cohort study of consecutively admitted acute medical patients.
The Acute Medical Unit, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark.
Acute medical patients admitted between November 18, 2013, and September 30, 2015.
None.
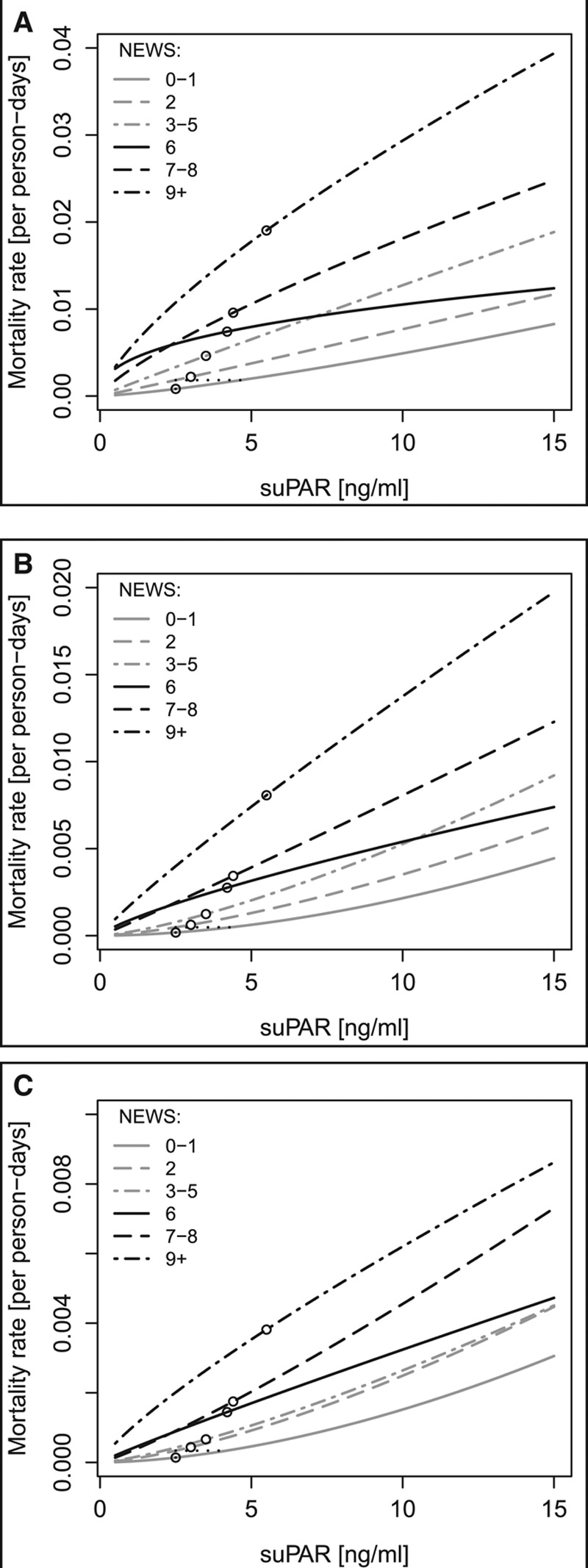
Of 17,312 included patients, admission National Early Warning Score was available for 16,244 (93.8%). During follow-up, 587 patients (3.4%) died in-hospital, 859 (5.0%) within 30 days, and 1,367 (7.9%) within 90 days. High soluble urokinase plasminogen activator receptor was significantly associated with in-hospital-, 30-day-, and 90-day mortality within all National Early Warning Score groups, in particular in patients with a low National Early Warning Score; for 30-day mortality, mortality rate ratios ranged from 3.45 (95% CI, 2.91-4.10) for patients with National Early Warning Score 0-1, to 1.86 (95% CI, 1.47-2.34) for patients with National Early Warning Score greater than or equal to 9 for every doubling in soluble urokinase plasminogen activator receptor (log2-transformed). Combining National Early Warning Score, age, and sex with soluble urokinase plasminogen activator receptor improved prediction of in-hospital-, 30-day-, and 90-day mortality, increasing the area under the curve (95% CI) for 30-day mortality from 0.86 (0.85-0.87) to 0.90 (0.89-0.91), p value of less than 0.0001, with a negative predictive value of 99.0%.
The addition of soluble urokinase plasminogen activator receptor to National Early Warning Score significantly improved risk prediction of both low- and high-risk acute medical patients. Patients with low National Early Warning Score but elevated soluble urokinase plasminogen activator receptor had mortality risks comparable to that of patients with higher National Early Warning Score.
可溶性尿激酶型纤溶酶原激活物受体是与危重病、疾病进展和死亡风险相关的预后生物标志物。我们旨在评估可溶性尿激酶型纤溶酶原激活物受体是否为急性内科患者临床监测风险的生命体征为基础的评分(国家早期预警评分)提供了额外的预后价值。
连续收治的急性内科患者的基于登记的观察性队列研究。
丹麦哥本哈根大学阿马格尔和维德霍夫医院的急性内科病房。
2013 年 11 月 18 日至 2015 年 9 月 30 日期间收治的急性内科患者。
无。
在纳入的 17312 例患者中,16244 例(93.8%)可获得入院时的国家早期预警评分。在随访期间,587 例(3.4%)患者住院期间死亡,859 例(5.0%)在 30 天内死亡,1367 例(7.9%)在 90 天内死亡。可溶性尿激酶型纤溶酶原激活物受体水平高与所有国家早期预警评分组的院内、30 天和 90 天死亡率显著相关,尤其是在国家早期预警评分较低的患者中;对于 30 天死亡率,死亡率比值范围从国家早期预警评分 0-1 的患者为 3.45(95%可信区间,2.91-4.10)到国家早期预警评分大于或等于 9 的患者为 1.86(95%可信区间,1.47-2.34)可溶性尿激酶型纤溶酶原激活物受体每增加一倍(对数 2 转换)。将国家早期预警评分、年龄和性别与可溶性尿激酶型纤溶酶原激活物受体结合,可改善院内、30 天和 90 天死亡率的预测,将 30 天死亡率的曲线下面积(95%可信区间)从 0.86(0.85-0.87)提高到 0.90(0.89-0.91),p 值小于 0.0001,阴性预测值为 99.0%。
可溶性尿激酶型纤溶酶原激活物受体与国家早期预警评分相结合,显著改善了低危和高危急性内科患者的风险预测。国家早期预警评分较低但可溶性尿激酶型纤溶酶原激活物受体升高的患者的死亡率风险与国家早期预警评分较高的患者相当。