From the Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts.
Department of Brain and Cognitive Science, Massachusetts Institute of Technology, Cambridge, Massachusetts.
Anesth Analg. 2018 Nov;127(5):1246-1258. doi: 10.1213/ANE.0000000000003668.
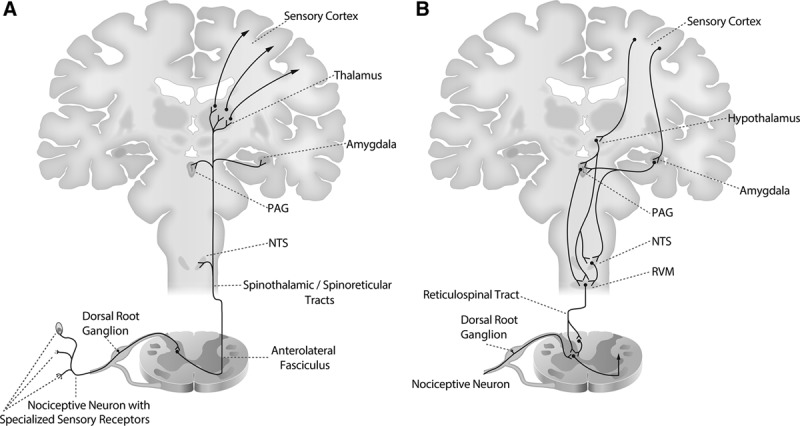
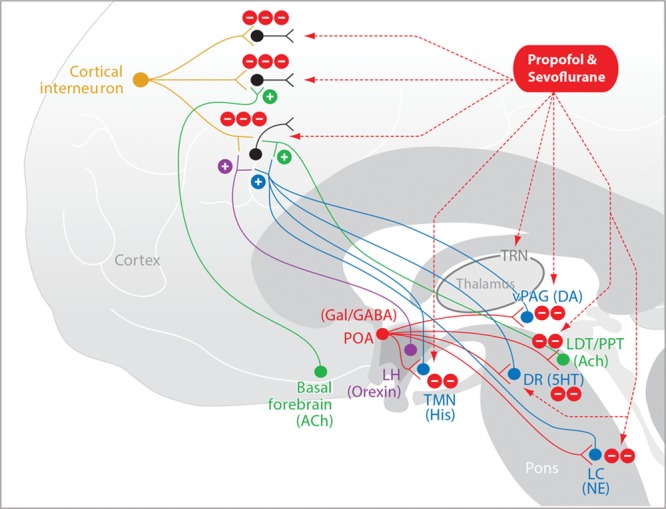
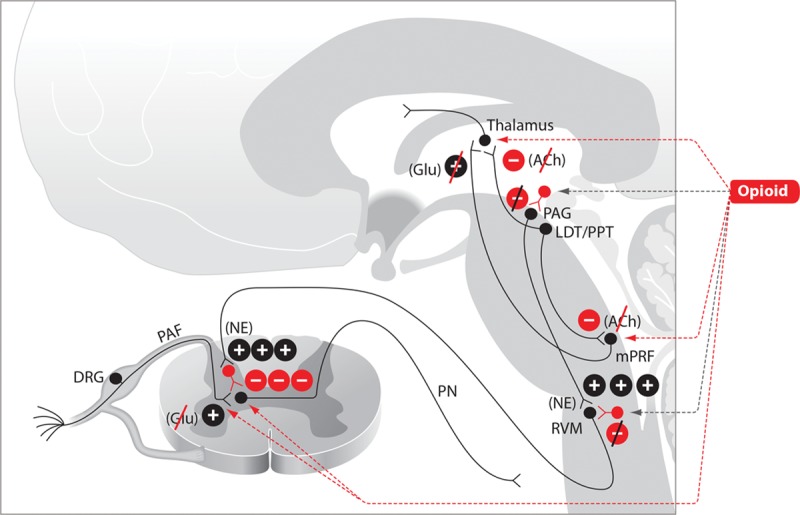
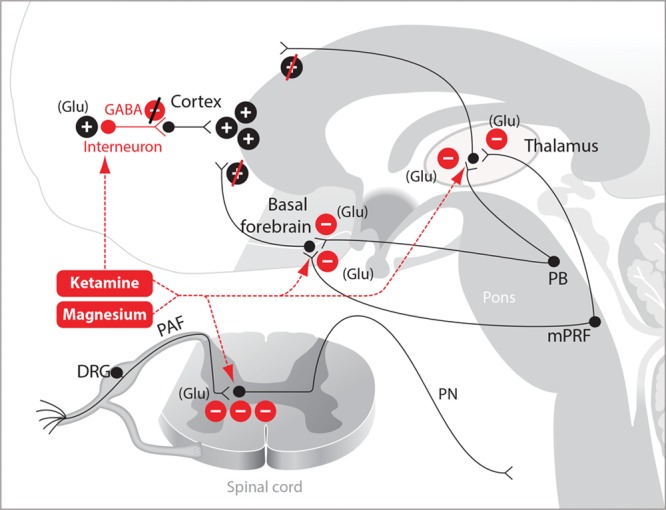
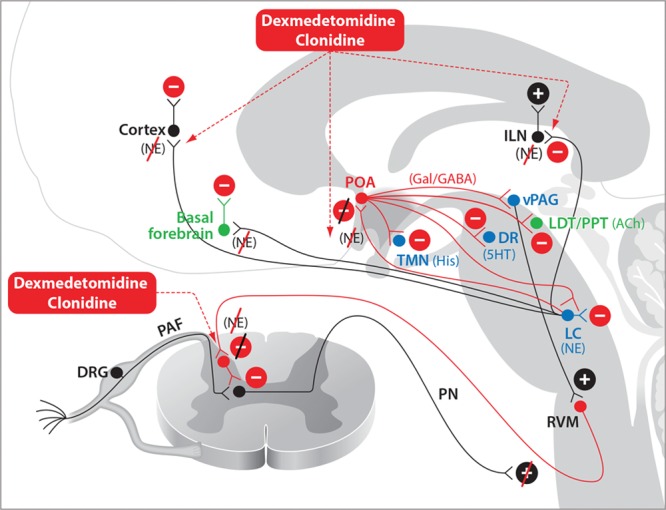
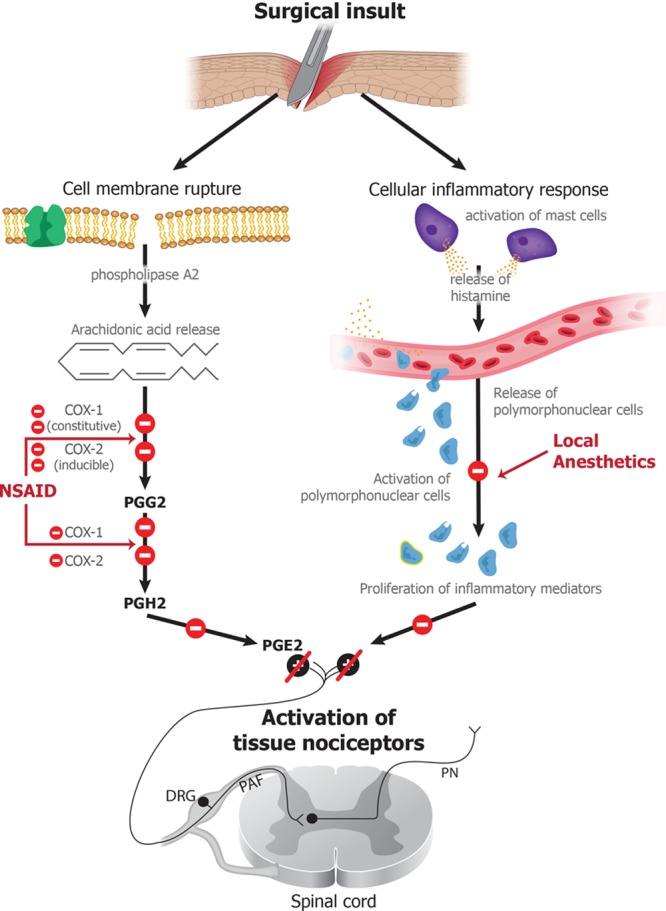
Balanced general anesthesia, the most common management strategy used in anesthesia care, entails the administration of different drugs together to create the anesthetic state. Anesthesiologists developed this approach to avoid sole reliance on ether for general anesthesia maintenance. Balanced general anesthesia uses less of each drug than if the drug were administered alone, thereby increasing the likelihood of its desired effects and reducing the likelihood of its side effects. To manage nociception intraoperatively and pain postoperatively, the current practice of balanced general anesthesia relies almost exclusively on opioids. While opioids are the most effective antinociceptive agents, they have undesirable side effects. Moreover, overreliance on opioids has contributed to the opioid epidemic in the United States. Spurred by concern of opioid overuse, balanced general anesthesia strategies are now using more agents to create the anesthetic state. Under these approaches, called "multimodal general anesthesia," the additional drugs may include agents with specific central nervous system targets such as dexmedetomidine and ones with less specific targets, such as magnesium. It is postulated that use of more agents at smaller doses further maximizes desired effects while minimizing side effects. Although this approach appears to maximize the benefit-to-side effect ratio, no rational strategy has been provided for choosing the drug combinations. Nociception induced by surgery is the primary reason for placing a patient in a state of general anesthesia. Hence, any rational strategy should focus on nociception control intraoperatively and pain control postoperatively. In this Special Article, we review the anatomy and physiology of the nociceptive and arousal circuits, and the mechanisms through which commonly used anesthetics and anesthetic adjuncts act in these systems. We propose a rational strategy for multimodal general anesthesia predicated on choosing a combination of agents that act at different targets in the nociceptive system to control nociception intraoperatively and pain postoperatively. Because these agents also decrease arousal, the doses of hypnotics and/or inhaled ethers needed to control unconsciousness are reduced. Effective use of this strategy requires simultaneous monitoring of antinociception and level of unconsciousness. We illustrate the application of this strategy by summarizing anesthetic management for 4 representative surgeries.
平衡全身麻醉是麻醉护理中最常用的管理策略,它涉及联合使用不同的药物来产生麻醉状态。麻醉师采用这种方法是为了避免仅仅依赖乙醚来维持全身麻醉。平衡全身麻醉使用的每种药物的剂量都比单独使用时少,从而增加了所需效果的可能性,并降低了副作用的可能性。为了在手术期间管理伤害感受和术后疼痛,目前平衡全身麻醉的做法几乎完全依赖阿片类药物。虽然阿片类药物是最有效的镇痛剂,但它们有不良的副作用。此外,过度依赖阿片类药物导致了美国的阿片类药物流行。由于担心阿片类药物的过度使用,平衡全身麻醉策略现在使用更多的药物来产生麻醉状态。在这些被称为“多模式全身麻醉”的方法中,额外的药物可能包括具有特定中枢神经系统靶点的药物,如右美托咪定,以及靶点不太明确的药物,如镁。据推测,使用较小剂量的更多药物可以进一步最大限度地发挥预期效果,同时最大限度地减少副作用。尽管这种方法似乎最大限度地提高了效益-副作用比,但对于选择药物组合,还没有提供合理的策略。手术引起的伤害感受是使患者处于全身麻醉状态的主要原因。因此,任何合理的策略都应侧重于手术期间的伤害感受控制和术后的疼痛控制。在这篇特稿中,我们回顾了伤害感受和觉醒回路的解剖学和生理学,以及常用的麻醉剂和麻醉辅助剂在这些系统中作用的机制。我们提出了一种基于选择作用于伤害感受系统不同靶点的药物组合来控制手术期间的伤害感受和术后疼痛的多模式全身麻醉的合理策略。由于这些药物也会降低觉醒,因此需要减少催眠药和/或吸入醚的剂量来控制无意识。这种策略的有效使用需要同时监测镇痛和无意识水平。我们通过总结 4 种代表性手术的麻醉管理来举例说明这种策略的应用。