Usher Institute of Population Health Sciences and Informatics, University of Edinburgh, Edinburgh, United Kingdom.
Institute for International Programs, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, USA.
J Glob Health. 2018 Dec;8(2):020807. doi: 10.7189/jogh.08.020807.
Traditionally, health care-seeking for child illness is assessed through population-based and nationally representative demographic and health surveys (DHS) that are conducted once every five to seven years and are based on maternal recall. These maternal reports are subject to recall bias. Mobile phones (with the use of GPS technology) have the potential to constantly track movements of phone owners and provide high quality and more accurate data at a population level in low and middle income countries (LMICs) to assess the validity of maternal recall. We provided a group of mothers with smartphones installed with a location-aware application and visited them monthly to administer a survey questionnaire on care-seeking for diarrhoea, fever and cough with fever. This paper assesses for any reactivity to smartphones or repeated study contacts for measuring care-seeking and if this resulted in change in health care provider preference.
We enrolled 749 mothers from rural areas of Pune district in Maharashtra, India and randomly allocated them to one of three groups - a longitudinal phone group, a longitudinal control group and a cross-sectional control group. We collected baseline information from mothers, including individual and household demographic and socio-economic characteristics and care-seeking preferences for child illness. We followed up both longitudinal groups monthly and each cross-sectional sub-group once over a period of 6 months. At each follow up, we administered questions identical to those in the National Family Health Survey (NFHS) questionnaire to determine an episode of diarrhoea, fever or cough within the last 15 days, care seeking for the same, and the type of provider. The data were analysed using the χ test or Fisher Exact Test for categorical variables, or with the Kruskall-Wallis non-parametric test for continuous variables (due to the non-normal nature of the data). Multivariable joint models of group and visit time were analysed with logistic regression methods.
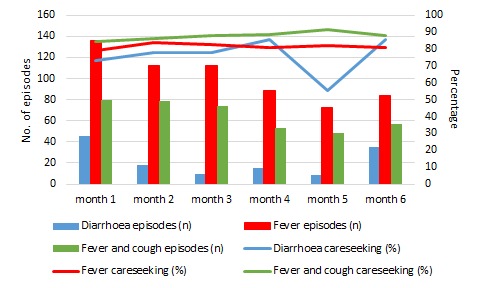
All three groups were similar in their socio-demographic characteristics at baseline. We did not observe any significant difference in care seeking for diarrhoea, fever or cough with fever between groups. Also, we did not observe any significant difference in proportion of children seeking care from the private sector.
We did not observe any reactivity in this study due to the presence of the phone (Hawthorne effect) or repeated study visits. The study also shows the potential of using GPS enabled smartphones to enrich DHS surveys in LMICs like India. However, further studies need to be conducted in other population groups before the findings can be generalised.
传统上,通过基于人群的、具有全国代表性的人口和健康调查(DHS)来评估儿童疾病的医疗保健寻求情况,这些调查每五到七年进行一次,并且基于产妇回忆。这些产妇报告易受回忆偏倚影响。移动电话(利用 GPS 技术)有可能不断跟踪电话所有者的行踪,并在中低收入国家(LMIC)以人群为基础提供高质量和更准确的数据,以评估产妇回忆的有效性。我们为一组母亲提供了安装有位置感知应用程序的智能手机,并每月访问她们,就腹泻、发热和咳嗽伴发热的医疗保健寻求情况进行调查。本文评估了智能手机或重复研究接触对医疗保健寻求的反应性,以及这是否导致医疗保健提供者偏好的变化。
我们从印度马哈拉施特拉邦浦那区的农村地区招募了 749 名母亲,并将她们随机分配到三个组之一:纵向手机组、纵向对照组和横向对照组。我们从母亲那里收集了基线信息,包括个人和家庭人口统计学和社会经济特征以及儿童疾病的医疗保健寻求偏好。我们每月随访两组纵向组,每六个月随访一次每个横向子组。在每次随访时,我们都会根据全国家庭健康调查(NFHS)问卷中的相同问题来确定过去 15 天内是否出现腹泻、发热或咳嗽、寻求同样的医疗保健服务以及提供者的类型。使用卡方检验或 Fisher 精确检验进行分类变量分析,或使用 Kruskal-Wallis 非参数检验进行连续变量分析(由于数据的非正态性质)。使用逻辑回归方法分析组和访问时间的多变量联合模型。
在基线时,所有三组在社会人口统计学特征方面均相似。我们没有观察到组间在腹泻、发热或咳嗽伴发热的医疗保健寻求方面存在任何显著差异。此外,我们也没有观察到儿童从私营部门寻求医疗保健的比例有任何显著差异。
在本研究中,由于电话的存在(霍桑效应)或重复的研究访问,我们没有观察到任何反应。该研究还展示了在印度等 LMIC 使用启用 GPS 的智能手机来丰富 DHS 调查的潜力。然而,在推广这些发现之前,还需要在其他人群中进行进一步的研究。