El-Agwany Ahmed Samy
Gyne-Oncology Specialized Center, Shatby Maternity University Hospital, Alexandria University, Alexandria, Egypt.
Gynecol Minim Invasive Ther. 2018 Apr-Jun;7(2):66-69. doi: 10.4103/GMIT.GMIT_1_17. Epub 2018 May 2.
Comprehensive staging laparotomy and cytoreductive surgery followed by chemotherapy has been the standard of care in advanced ovarian cancer. Neoadjuvant chemotherapy is an alternative in inoperable advanced cases. To select patients amenable for successful cytoreduction, major determinants including CT imaging and laparoscopy could be of value. There is no general accepted model for selection and reproducibility of techniques are a major challenge due to different clinical practice and complexity of scoring systems. Some lesions as small size (<5 mm) peritoneal deposits and mesenteric affection are hard to see on CT so, complementary laparoscopy may play a role in the preoperative assessment. The aim of this study was evaluation of the role of laparoscopy in advanced ovarian tumors for prediction of optimal cytoreductive surgery in relation to CT and surgical peritoneal carcinomatosis index (PCI).
Was to evaluate laparoscopic assessment in advanced ovarian tumors for prediction of optimal cytoreductive surgery in relation to CT and surgical peritoneal carcinomatosis index (PCI).
Gyne-oncology specialized center, El-Shatby maternity university hospital, Alexandria Egypt.
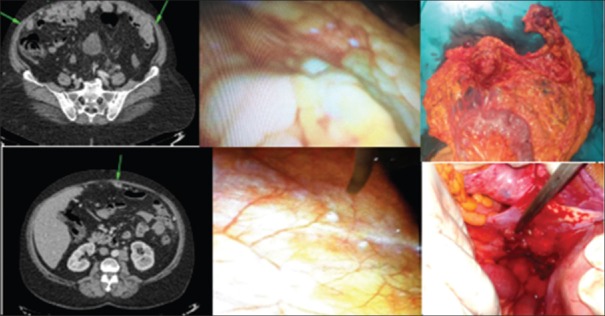
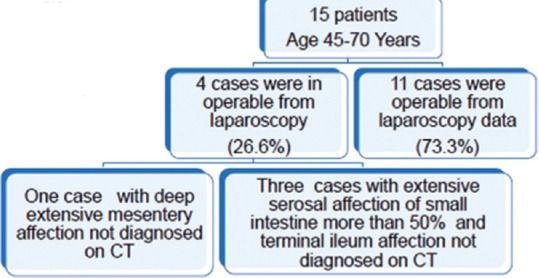
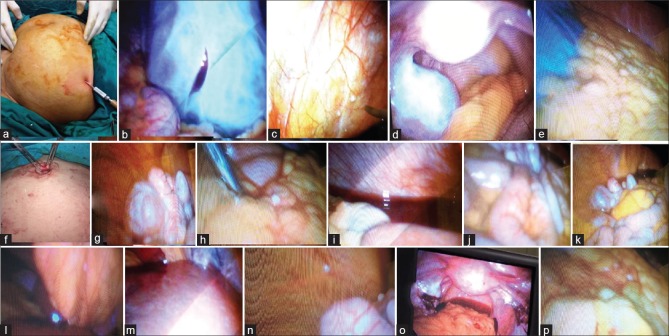
From January 2016 to December 2016, 15 patients were recruited from gyne-oncology specialized center, Alexandria, Egypt. Patients underwent a special design described later then laparoscopy using palmar point entry was done for assessing small lesions and the extent of affection in surface peritoneal, mesentery, serosa of the gut especially small intestine (terminal ileum affection, more or less than 50% affection) mainly with evaluating other sites as liver surface and diaphragm peritoneal surface affection after removal of ascites by aspiration. Findings were correlated with laparotomy and CT scan findings. Surgery was performed in the same setting which is better or with in two weeks.
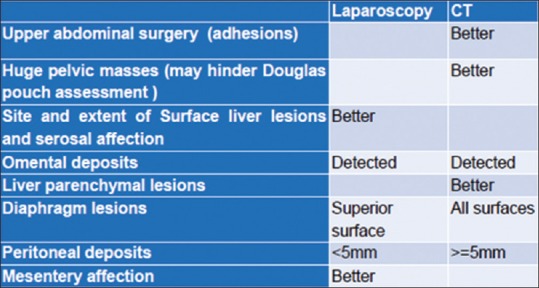
There were two cases with upper abdominal surgeries (cholecystectomy and splenectomy) where no visualization of liver and stomach on laparoscopy but were free on CT scan and surgical evaluation. Douglas pouch was not assessed in two patients with large fixed bilateral ovarian masses on laparoscopy. Two cases with diaphragmatic affection on CT scan related to the posterior surface were not detected on laparoscopy. These findings were correlated with surgical findings as the gold standard. The pathology was ranging from low grade to high grade serous cyst adenocarcinoma.
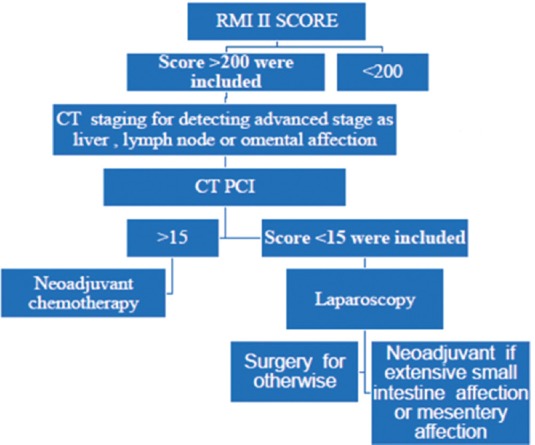
Laparoscopic evaluation is a useful adjunct with CT prior to performing ovarian cancer cytoreductive surgery for assessment of operability. Laparoscopy is better for evaluating extent of serosal affection in advanced tumors in cases with omental cakes on CT. A roadmap for prediction of operability in advanced ovarian cancer can be used by combing CT PCI and laparoscopic assessment.
全面分期剖腹术和肿瘤细胞减灭术随后进行化疗一直是晚期卵巢癌的标准治疗方法。新辅助化疗是无法手术的晚期病例的一种替代方案。为了选择适合成功进行肿瘤细胞减灭术的患者,包括CT成像和腹腔镜检查在内的主要决定因素可能具有价值。由于不同的临床实践和评分系统的复杂性,目前尚无普遍接受的选择模型,技术的可重复性是一个主要挑战。一些小尺寸(<5mm)的腹膜种植和肠系膜受累病变在CT上很难看到,因此,辅助腹腔镜检查可能在术前评估中发挥作用。本研究的目的是评估腹腔镜检查在晚期卵巢肿瘤中的作用,以预测与CT和手术腹膜癌指数(PCI)相关的最佳肿瘤细胞减灭术。
评估腹腔镜检查在晚期卵巢肿瘤中的作用,以预测与CT和手术腹膜癌指数(PCI)相关的最佳肿瘤细胞减灭术。
埃及亚历山大市埃尔-沙特比妇产大学医院妇科肿瘤专科中心。
2016年1月至2016年12月,从埃及亚历山大市的妇科肿瘤专科中心招募了15名患者。患者接受了稍后描述的特殊设计,然后采用掌式穿刺点入路进行腹腔镜检查,以评估小病变以及表面腹膜、肠系膜、肠道浆膜(尤其是小肠,回肠末端受累情况,受累程度大于或小于50%)的受累范围,主要是在通过抽吸去除腹水后评估其他部位,如肝表面和膈肌腹膜表面受累情况。将检查结果与剖腹术和CT扫描结果进行关联。手术在同一环境下进行,情况较好时在两周内进行。
有2例患者进行了上腹部手术(胆囊切除术和脾切除术),腹腔镜检查时未观察到肝脏和胃,但CT扫描和手术评估显示无病变。腹腔镜检查时,2例双侧卵巢巨大固定肿块的患者未评估Douglas窝。CT扫描显示2例膈肌后表面受累的病例在腹腔镜检查中未被发现。这些结果与作为金标准的手术结果相关。病理类型从低级别到高级别浆液性囊腺癌不等。
在进行卵巢癌肿瘤细胞减灭术之前,腹腔镜评估是CT检查的有用辅助手段,可用于评估手术可行性。对于CT显示有网膜饼的晚期肿瘤病例,腹腔镜检查在评估浆膜受累程度方面更好。结合CT PCI和腹腔镜评估,可以制定晚期卵巢癌手术可行性的预测路线图。