Zellweger Raphaël M, Basnyat Buddha, Shrestha Poojan, Prajapati Krishna G, Dongol Sabina, Sharma Paban K, Koirala Samir, Darton Thomas C, Boinett Christine, Thompson Corinne N, Thwaites Guy E, Baker Stephen, Karkey Abhilasha
Wellcome Trust Major Overseas Programme, Oxford University Clinical Research Unit, The Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam.
Oxford University Clinical Research Unit, Patan Academy of Health Sciences, Kathmandu, Nepal.
Front Med (Lausanne). 2018 Sep 19;5:262. doi: 10.3389/fmed.2018.00262. eCollection 2018.
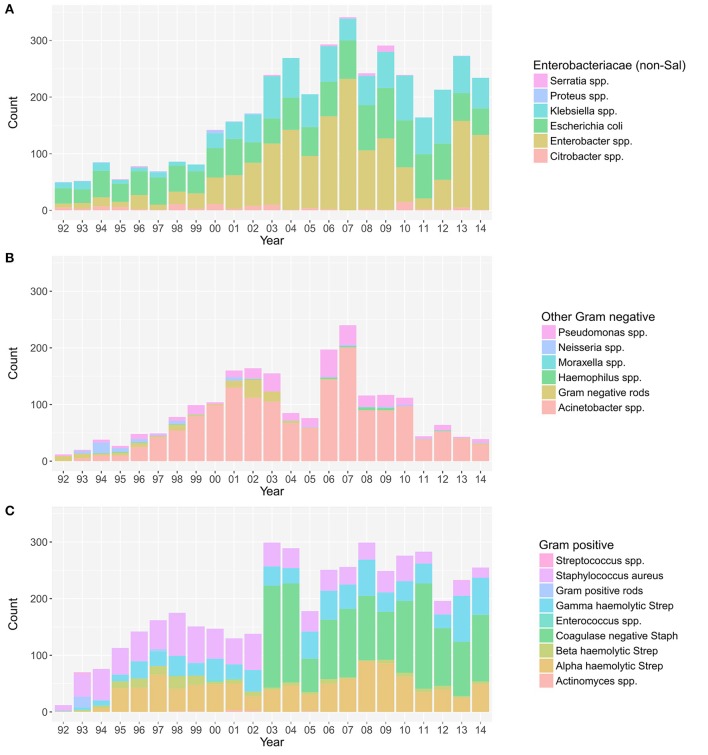
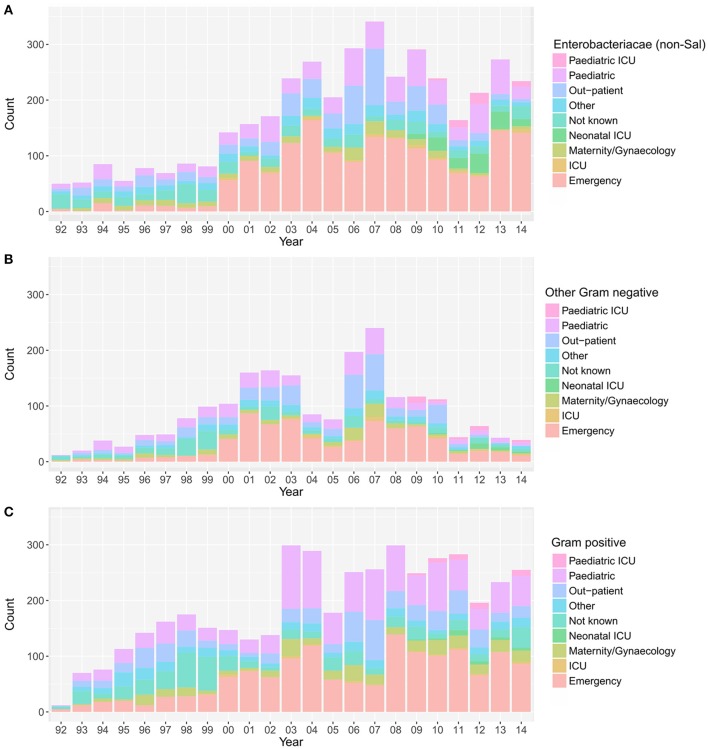
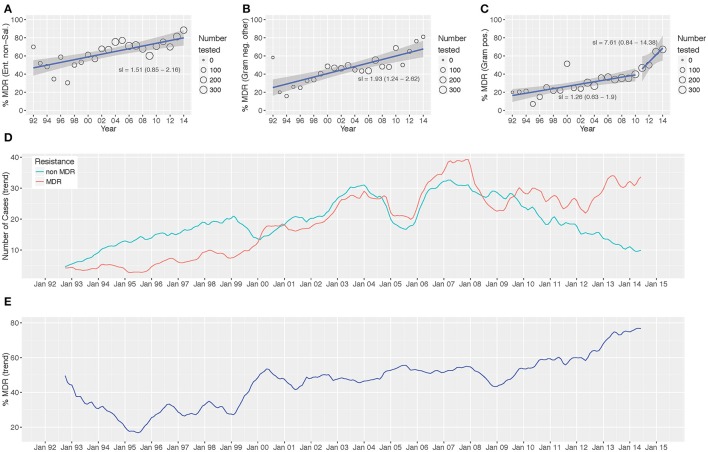
A comprehensive longitudinal understanding of the changing epidemiology of the agents causing bacteraemia and their AMR profiles in key locations is crucial for assessing the progression and magnitude of the global AMR crisis. We performed a retrospective analysis of routine microbiological data from April 1992 to December 2014, studying the time trends of non- associated bacteraemia at a single Kathmandu healthcare facility. The distribution of aetiological agents, their antimicrobial susceptibility profiles, and the hospital ward of isolation were assessed. Two hundred twenty-four thousand seven hundred forty-one blood cultures were performed over the study period, of which, 30,353 (13.5%) exhibited growth for non-contaminant bacteria. We observed a significant increasing trend in the proportion of MDR non- Enterobacteriaceae ( < 0.001), other Gram-negative organisms ( = 0.006), and Gram-positive organisms ( = 0.006) over time. Additionally, there was an annual increasing trend in the proportion of MDR organisms in bacteria-positive blood cultures originating from patients attending the emergency ward ( = 0.006) and the outpatient department ( = 0.006). This unique dataset demonstrates that community acquired non- bacteraemia has become an increasingly important cause of hospital admission in Kathmandu. An increasing burden of bacteraemia associated with MDR organisms in the community underscores the need for preventing the circulation of MDR bacteria within the local population.
全面纵向了解关键地区引起菌血症的病原体流行病学变化及其抗菌药物耐药性概况,对于评估全球抗菌药物耐药性危机的进展和严重程度至关重要。我们对1992年4月至2014年12月的常规微生物学数据进行了回顾性分析,研究了加德满都一家医疗机构中非相关性菌血症的时间趋势。评估了病原体的分布、其抗菌药物敏感性概况以及分离的医院病房。在研究期间共进行了224741次血培养,其中30353次(13.5%)培养出非污染性细菌。我们观察到,随着时间的推移,多重耐药非肠杆菌科细菌(<0.001)、其他革兰氏阴性菌(=0.006)和革兰氏阳性菌(=0.006)的比例呈显著上升趋势。此外,来自急诊科(=0.006)和门诊部(=0.006)患者的细菌阳性血培养中多重耐药菌的比例呈逐年上升趋势。这个独特的数据集表明,社区获得性非菌血症已成为加德满都医院入院的一个日益重要的原因。社区中与多重耐药菌相关的菌血症负担不断增加,凸显了防止多重耐药菌在当地人群中传播的必要性。