Department of Radiotherapy and Radiooncology, Medical Faculty, Heinrich Heine University, Moorenstr. 5, 40225, Dusseldorf, Germany.
Department of Oto-Rhino-Laryngology, Head and Neck Surgery, Ulm University Medical Center, Ulm, Germany.
Radiat Oncol. 2018 Oct 4;13(1):195. doi: 10.1186/s13014-018-1133-8.
Adjuvant radiotherapy in advanced head and neck squamous cell cancer (HNSCC) reduces the risk of local-regional failure and most likely increases the survival rate. Patients at high risk for tumor recurrence may benefit from more aggressive altered fractionation schedules in order to reduce the overall time from surgery to completion of radiotherapy. Here, we reviewed the results of six randomized trials addressing the above hypothesis.
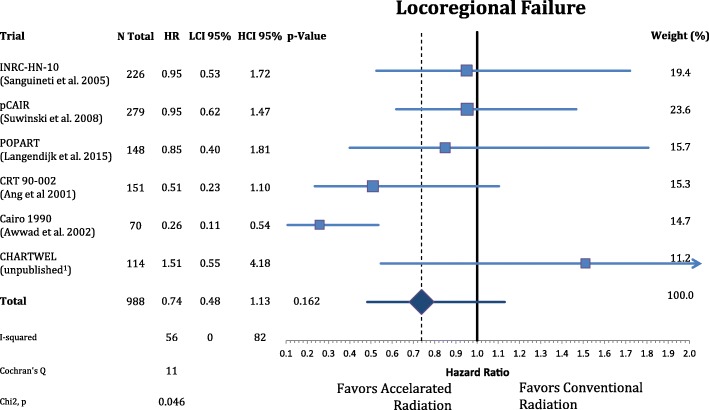
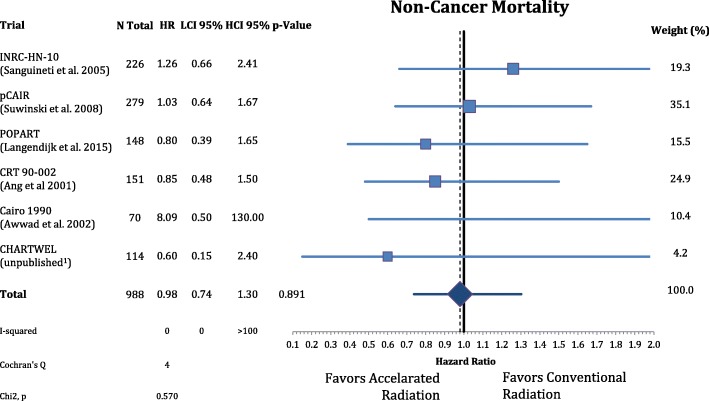
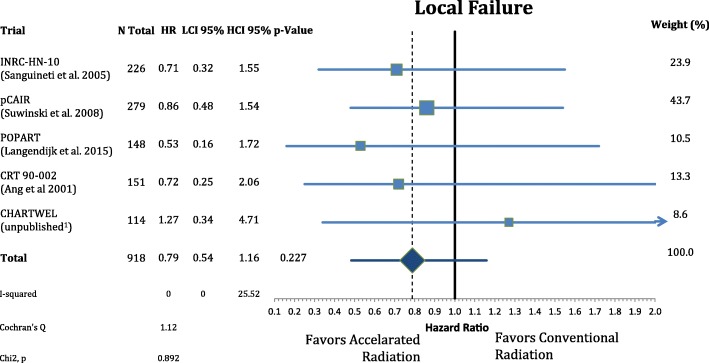
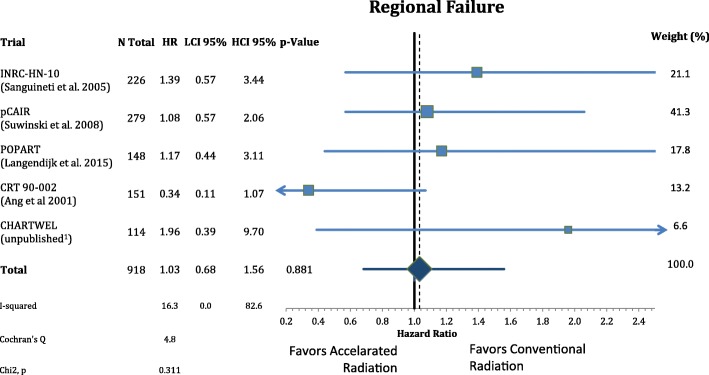
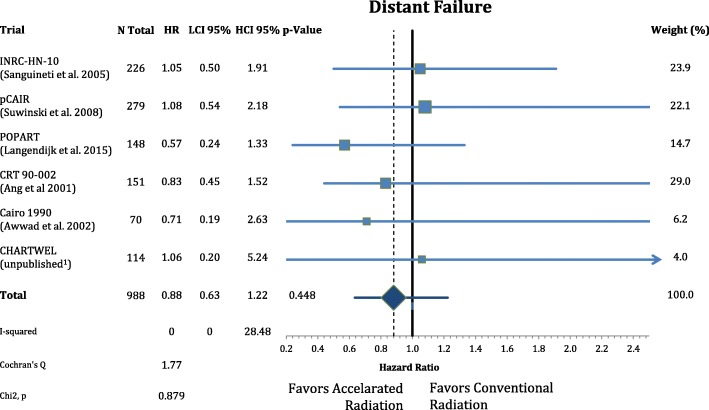
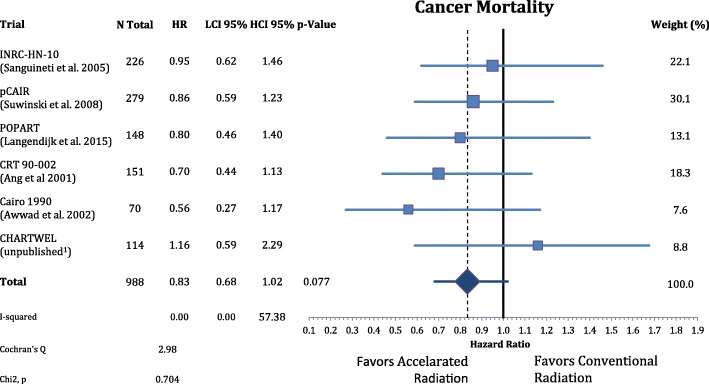
In the six trials of interest, a total of 988 patients with locally advanced HNSCC were randomly assigned to receive either accelerated or conventionally fractionated adjuvant radiotherapy. Hazard ratios (HR) were extracted from available publications for local-regional control, distant metastasis as well as overall-, cancer specific- and disease-free survival. Meta-analysis of the effect sizes was performed using fixed and random effect models. Acute and late side effects were categorized and summarized for comparison.
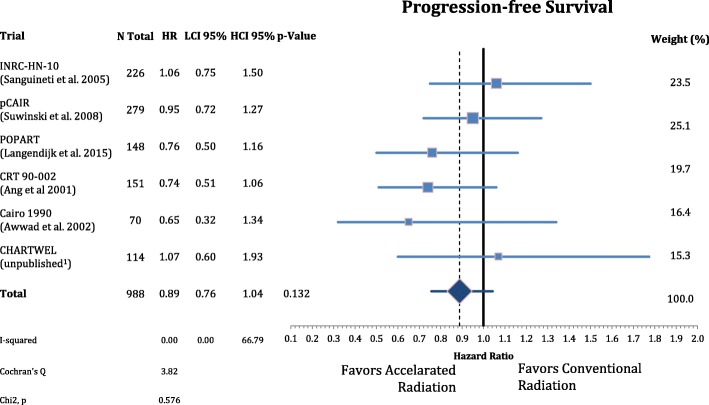
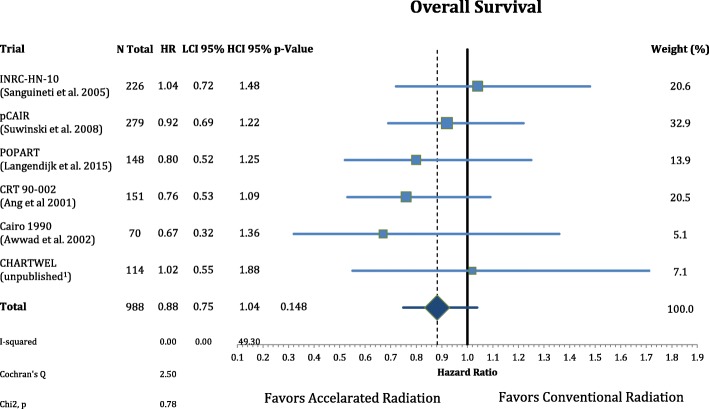
Accelerated radiotherapy did not improve the loco-regional control (n = 988, HR = 0.740, CI = 0.48-1.13, p = 0.162), progression-free survival (HR = 0.89, CI = 0.76-1.04, p = 0.132) or overall survival (HR = 0.88, CI = 0.75-1.04, p = 0.148) significantly. Acute confluent mucositis occurred with significant higher frequency with accelerated radiotherapy. Late side effects did not differ significantly in either group.
Accelerated radiotherapy does not result in a significant improvement of loco-regional control or overall survival in high-risk patients. Acute but not late radiation toxicity were more frequent with the accelerated RT technique. In clinical practice accelerated postoperative radiation therapy might be a suitable option only for a subset of patients.
在晚期头颈部鳞状细胞癌(HNSCC)中进行辅助放疗可降低局部区域失败的风险,并且很可能提高生存率。肿瘤复发风险高的患者可能受益于更积极的改变分割方案,以减少从手术到放疗完成的总时间。在这里,我们回顾了六项针对上述假设的随机试验的结果。
在六个相关试验中,共有 988 名局部晚期 HNSCC 患者被随机分配接受加速或常规分割辅助放疗。从可用文献中提取局部区域控制、远处转移以及总体、癌症特异性和无病生存率的风险比(HR)。使用固定和随机效应模型对效应大小进行荟萃分析。对急性和晚期副作用进行分类和总结以进行比较。
加速放疗并未改善局部区域控制(n=988,HR=0.740,CI=0.48-1.13,p=0.162)、无进展生存率(HR=0.89,CI=0.76-1.04,p=0.132)或总生存率(HR=0.88,CI=0.75-1.04,p=0.148)。加速放疗后,急性融合性黏膜炎的发生率显著升高。两组的晚期副作用无明显差异。
在高危患者中,加速放疗并未显著改善局部区域控制或总体生存率。加速 RT 技术的急性但非晚期放射毒性更频繁。在临床实践中,加速术后放疗可能仅适用于一部分患者。