Josephs Michael, Bayard Dominique, Gabler Nicole B, Cooney Elizabeth, Halpern Scott D
Fostering Improvement in End-of-Life Decision Science Program (MJ, NBG, EC, SDH), Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.
Division of Pulmonary, Allergy and Critical Care Medicine (SDH), Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.
MDM Policy Pract. 2018 Feb 20;3(1):2381468317753127. doi: 10.1177/2381468317753127. eCollection 2018 Jan-Jun.
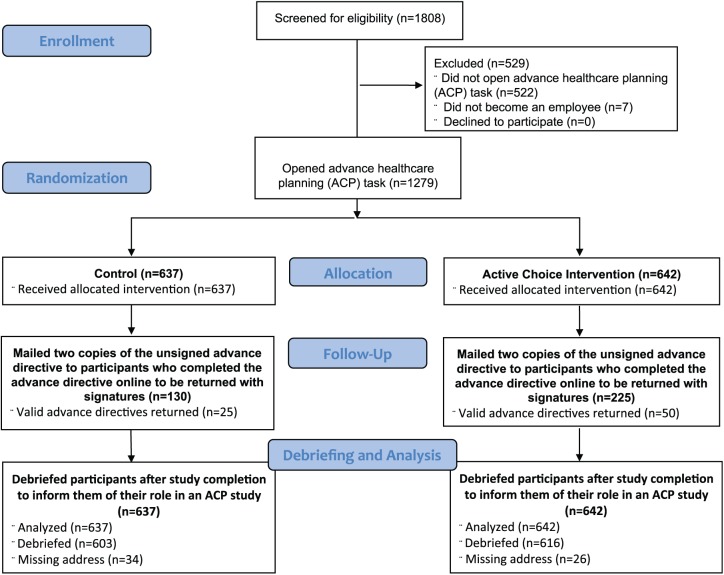
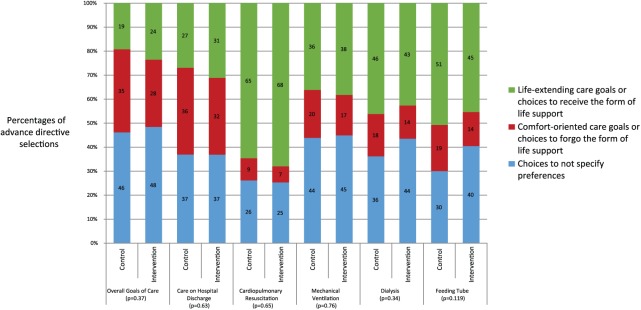
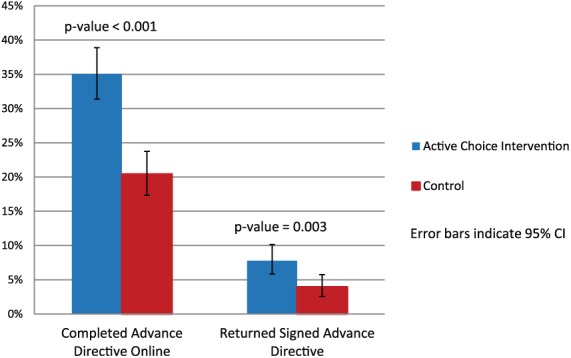
Many people recognize the potential benefits of advance directives (ADs), yet few actually complete them. It is unknown whether an active choice intervention influences AD completion. New employees were randomized to an active choice intervention (n = 642) or usual care (n = 637). The active choice intervention asked employees to complete an AD, confirm prior AD completion, or fill out a declination form. In usual care, participants could complete an AD, confirm prior completion, or skip the task. We used multivariable logistic regression to assess the relationship between the intervention arm and both AD completion online and the return of a signed AD by mail, as well as assess interactions between intervention group and age, gender, race, and clinical degree status. Participants assigned to the active choice intervention more commonly completed ADs online (35.1% v. 20.4%, P < 0.001) (odds ratio [OR] = 2.10; 95% confidence interval [CI] = 1.63-2.71; number needed to treat = 6.8) and returned signed ADs by mail (7.8% v. 3.9%, P = 0.003; number needed to treat = 25.6). The effect of the intervention was significantly greater among men (OR = 4.13; 95% CI = 2.32-7.35) than among women (OR = 1.74; 95% CI = 1.30-2.32) (interaction P value < 0.001). Responses to all eight choices made in the ADs were similar between groups (all P > 0.10). A young and healthy participant may not benefit from AD completion as an older or seriously ill patient would. The active choice intervention significantly increased the proportion of participants completing an AD without changing the choices in ADs. This relationship was especially strong among men and may be a useful method to increase AD completion rates without altering choices.
许多人认识到预先医疗指示(ADs)的潜在益处,但实际完成的人却很少。尚不清楚积极选择干预措施是否会影响预先医疗指示的完成情况。新员工被随机分为积极选择干预组(n = 642)或常规护理组(n = 637)。积极选择干预措施要求员工完成一份预先医疗指示、确认之前已完成的预先医疗指示或填写一份拒绝表格。在常规护理中,参与者可以完成一份预先医疗指示、确认之前已完成的指示或跳过该任务。我们使用多变量逻辑回归来评估干预组与在线完成预先医疗指示以及通过邮件返还签署的预先医疗指示之间的关系,并评估干预组与年龄、性别、种族和临床学位状态之间的相互作用。被分配到积极选择干预组的参与者更常在线完成预先医疗指示(35.1%对20.4%,P < 0.001)(比值比[OR] = 2.10;95%置信区间[CI] = 1.63 - 2.71;需治疗人数 = 6.8),并且通过邮件返还签署的预先医疗指示(7.8%对3.9%,P = 0.003;需治疗人数 = 25.6)。干预措施对男性的影响(OR = 4.13;95% CI = 2.32 - 7.35)显著大于女性(OR = 1.74;95% CI = 1.30 - 2.32)(相互作用P值 < 0.001)。两组对预先医疗指示中所有八个选项的回答相似(所有P > 0.10)。年轻健康的参与者可能不会像年长或重病患者那样从完成预先医疗指示中受益。积极选择干预措施显著提高了完成预先医疗指示的参与者比例,但未改变预先医疗指示中的选项。这种关系在男性中尤为明显,可能是一种在不改变选项的情况下提高预先医疗指示完成率的有用方法。