Gupta Sonali, Goyal Pradeep, Sharma Pranav, Soin Priti, Kochar Puneet S
Department of Medicine, St. Vincent's Medical Center, Bridgeport, CT, USA.
The Frank H. Netter MD School of Medicine at Quinnipiac University, North Haven, CT, USA.
Ann Med Surg (Lond). 2018 Sep 13;35:141-145. doi: 10.1016/j.amsu.2018.09.003. eCollection 2018 Nov.
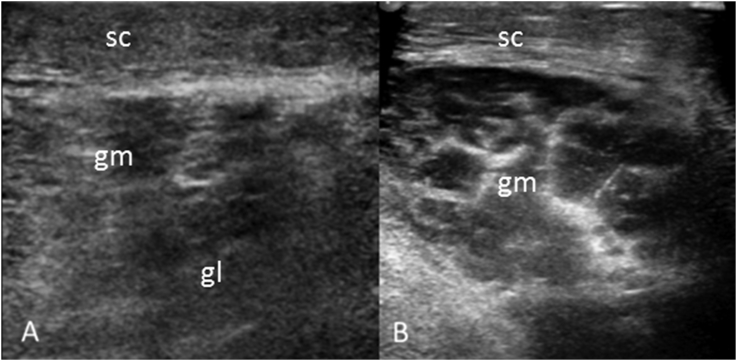
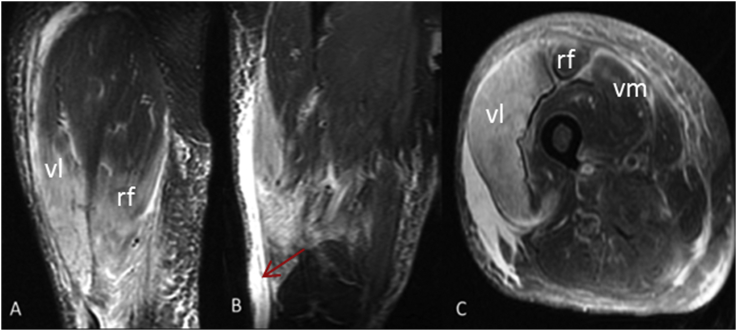
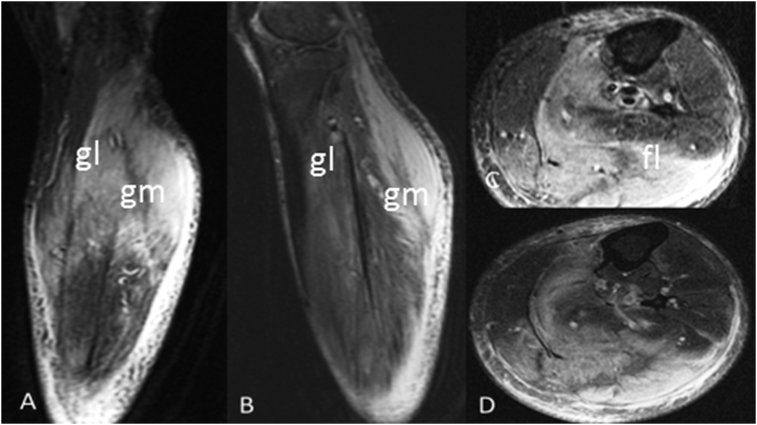
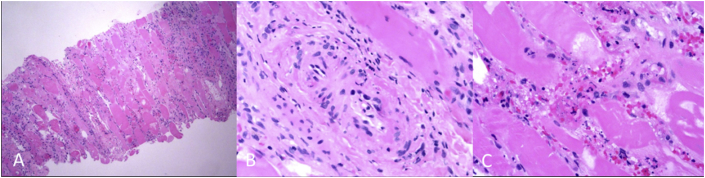
Diabetic myonecrosis (DMN) is an under-diagnosed complication of long-standing poorly controlled diabetes mellitus. It presents as abrupt pain and swelling of the extremity, mostly lower limbs. Diagnosis is often delayed as it mimics a number of clinical entities such as deep vein thrombosis (DVT), cellulitis, necrotizing fasciitis and malignancy. Failure to properly identify this condition can result in increased morbidity through exposure to unnecessary tests and biopsy. A 56-year-old male with a history of complicated type 2 diabetes mellitus, hypertension presented to emergency with gradually worsening left calf pain for last 2 weeks. A lower-extremity venous Doppler was negative for DVT. Magnetic resonance imaging (MRI) was suggestive of muscle edema likely of inflammatory etiology. Muscle biopsy revealed myonecrosis with ischemic myopathy and was negative for vasculitis or inflammatory myopathy. He was managed conservatively and his symptoms resolved in 4 weeks. After 6 months he had recurrence in right thigh which was managed conservatively too. Given these findings, a diagnosis of recurrent diabetic myonecrosis was made. Myonecrosis is a less known microvascular complications of diabetes and should always be keep in mind when evaluating a diabetic patient with muscle pain. Diagnosis can be made on MRI in appropriate clinical settings. The clinical course is usually self-limiting and patients respond well to supportive medical therapy that involves bed rest, strict glycemic control along with analgesic.
糖尿病性肌坏死(DMN)是长期血糖控制不佳的糖尿病一种诊断不足的并发症。其表现为肢体突然疼痛和肿胀,多数发生在下肢。由于它可模仿多种临床病症,如深静脉血栓形成(DVT)、蜂窝织炎、坏死性筋膜炎和恶性肿瘤,故诊断常被延误。未能正确识别这种病症可能会因接受不必要的检查和活检而导致发病率增加。一名56岁男性,有2型糖尿病、高血压病史,因左小腿疼痛在过去2周逐渐加重而就诊于急诊科。下肢静脉多普勒检查显示DVT阴性。磁共振成像(MRI)提示可能为炎症性病因的肌肉水肿。肌肉活检显示为伴有缺血性肌病的肌坏死,血管炎或炎性肌病检查结果为阴性。他接受了保守治疗,症状在4周内缓解。6个月后,他右大腿复发,同样接受了保守治疗。基于这些发现,诊断为复发性糖尿病性肌坏死。肌坏死是一种较少为人所知的糖尿病微血管并发症,在评估有肌肉疼痛的糖尿病患者时应始终牢记。在适当的临床情况下,可通过MRI做出诊断。临床病程通常为自限性,患者对包括卧床休息、严格血糖控制以及镇痛在内的支持性药物治疗反应良好。