Jo So Yoon, Lee Chan-Ho, Jung Woo-Jin, Kim Sung-Won, Hwang Yoon-Ha
Department of Pediatrics, Busan St. Mary's Hospital, Busan, Korea.
Korean J Pediatr. 2018 Nov;61(11):348-354. doi: 10.3345/kjp.2018.06324. Epub 2018 Sep 16.
The purpose of this study was to identify the causes, symptoms, and complications of hypoproteinemia to prevent hypoproteinemia and provide appropriate treatment to children with atopic dermatitis.
Children diagnosed with atopic dermatitis with hypoproteinemia and/or hypoalbuminemia were retrospectively reviewed. The patients' medical records, including family history, weight, symptoms, treatment, complications, and laboratory test results for allergies and skin cultures, were examined.
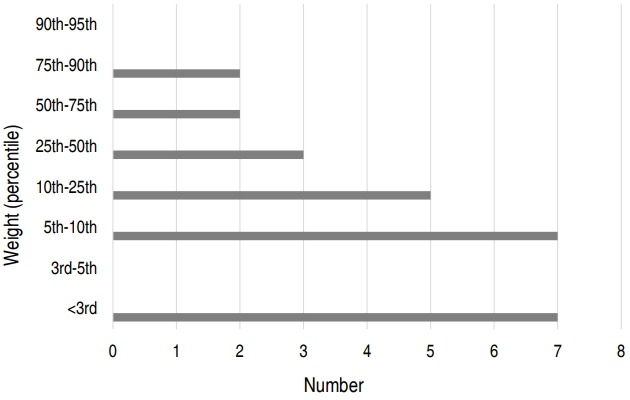
Twenty-six patients (24 boys) were enrolled. Seven cases had growth retardation; 7, keratoconjunctivitis; 6, aural discharges; 5, eczema herpeticum; 4, gastrointestinal tract symptoms; and 2, developmental delays. In 21 cases, topical steroids were not used. According to the blood test results, the median values of each parameter were elevated: total IgE, 1,864 U/mL; egg white-specific IgE, 76.5 kUA/L; milk IgE, 20.5 kUA/L; peanut IgE, 30 kUA/L; eosinophil count, 5,810/μL; eosinophil cationic protein, 93.45 μg/L; and platelet count, 666.5×103/μL. Serum albumin and total protein levels decreased to 2.7 g/dL and 4.25 g/dL, respectively. Regarding electrolyte abnormality, 10 patients had hyponatremia, and 12, hyperkalemia. Systemic antibiotics were used to treat all cases, and an antiviral agent was used in 12 patients. Electrolyte correction was performed in 8 patients.
Hypoproteinemia accompanying atopic dermatitis is common in infants younger than 1 year and may occur because of topical steroid treatment continuously being declined or because of eczema herpeticum. It may be accompanied by growth retardation, keratoconjunctivitis, aural discharge, and eczema herpeticum and can be managed through skin care and topical steroid application without intravenous albumin infusion.
本研究旨在确定低蛋白血症的病因、症状和并发症,以预防低蛋白血症,并为特应性皮炎患儿提供适当治疗。
对诊断为特应性皮炎合并低蛋白血症和/或低白蛋白血症的儿童进行回顾性研究。检查患者的病历,包括家族史、体重、症状、治疗、并发症以及过敏和皮肤培养的实验室检查结果。
共纳入26例患者(24例男孩)。7例有生长发育迟缓;7例有角结膜炎;6例有耳溢液;5例有疱疹样湿疹;4例有胃肠道症状;2例有发育迟缓。21例未使用外用类固醇。根据血液检查结果,各参数的中位数均升高:总IgE为1864 U/mL;蛋清特异性IgE为76.5 kUA/L;牛奶IgE为20.5 kUA/L;花生IgE为30 kUA/L;嗜酸性粒细胞计数为5810/μL;嗜酸性粒细胞阳离子蛋白为93.45 μg/L;血小板计数为666.5×10³/μL。血清白蛋白和总蛋白水平分别降至2.7 g/dL和4.25 g/dL。关于电解质异常,10例患者有低钠血症,12例有高钾血症。所有病例均使用全身抗生素治疗,12例患者使用了抗病毒药物。8例患者进行了电解质纠正。
特应性皮炎伴发的低蛋白血症在1岁以下婴儿中很常见,可能是由于持续减少外用类固醇治疗或疱疹样湿疹所致。它可能伴有生长发育迟缓、角结膜炎、耳溢液和疱疹样湿疹,可通过皮肤护理和外用类固醇应用进行管理,无需静脉输注白蛋白。