Department of Pulmonology, Pontíficia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil.
Department of Radiology, Irmandade Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, RS, Brazil.
PLoS One. 2018 Oct 11;13(10):e0205273. doi: 10.1371/journal.pone.0205273. eCollection 2018.
To evaluate the quantitative computed tomography (QCT) phenotypes, airflow limitations, and exacerbation-like episodes in heavy smokers in Southern Brazil.
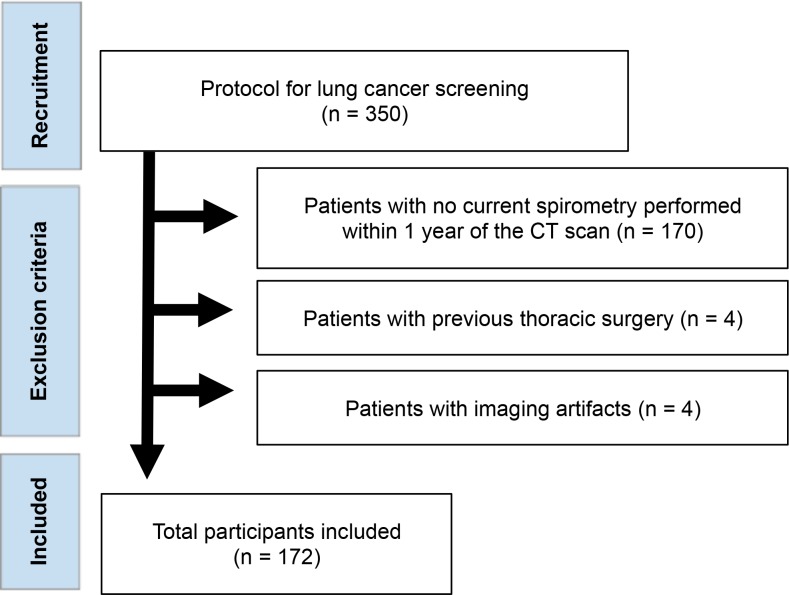
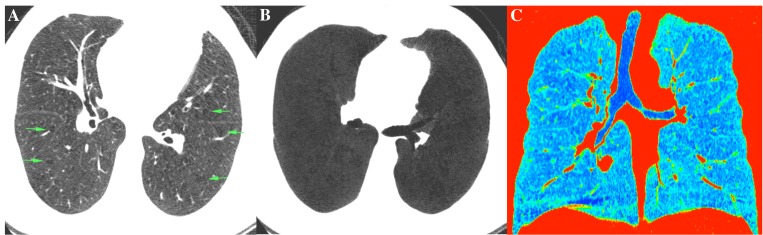
We enrolled 172 smokers with a smoking history ≥30 pack-years who underwent pulmonary function tests (PFTs) and CT scan for lung cancer screening. Patients were classified regarding airflow limitation (FEV1/FVC <0.7 forced expiratory volume in 1 second/forced vital capacity) and the presence of emphysema on the QCT. The QCT were analyzed in specialized software and patients were classified in two disease-predominant phenotypes: emphysema-predominant (EP) and non-emphysema-predominant (NEP). EP was determined as ≥6% of percent low-attenuation areas (LAA%) with less than -950 Hounsfield units. NEP was defined as having a total LAA% of less than 6%.
Most of our patients were classified in the EP phenotype. The EP group had significantly worse predicted FEV1 (60.6 ±22.9 vs. 89.7 ±15.9, p <0.001), higher rates of airflow limitation (85.7% vs. 15%; p <0.001), and had more exacerbation-like episodes (25.8% vs. 8.3%, p <0.001) compared to the NEP group. Smoking history, ethnicity, and BMI did not differ between the groups. The total LAA% was the QCT parameter with the strongest correlation to FEV1 (r = -0.669) and FEV1/FVC (r = -0.787).
Heavy smokers with the EP phenotype on QCT were more likely to have airflow limitation, worse predicted FEV1, and a higher rate of exacerbation-like episodes than those with the NEP phenotype. Approximately 23% of patients with no airflow limitation on PFTs were classified in EP phenotype.
评估南里奥格兰德州重度吸烟者的定量 CT(QCT)表型、气流受限和类似加重发作情况。
我们招募了 172 名吸烟史≥30 包年的吸烟者,他们接受了肺功能测试(PFT)和肺癌筛查 CT 扫描。根据气流受限(FEV1/FVC<0.7 秒第一秒用力呼气量/用力肺活量)和 QCT 上肺气肿的存在对患者进行分类。使用专门的软件对 QCT 进行分析,将患者分为两种以疾病为主的表型:肺气肿为主型(EP)和非肺气肿为主型(NEP)。EP 定义为≥6%的低衰减区(LAA%),且低于-950 亨氏单位。NEP 定义为总 LAA%低于 6%。
我们的大多数患者被归类为 EP 表型。EP 组的预计 FEV1 明显更差(60.6±22.9 与 89.7±15.9,p<0.001),气流受限率更高(85.7%与 15%;p<0.001),类似加重发作次数更多(25.8%与 8.3%;p<0.001)与 NEP 组相比。吸烟史、种族和 BMI 在两组之间无差异。总 LAA%是与 FEV1(r=-0.669)和 FEV1/FVC(r=-0.787)相关性最强的 QCT 参数。
与 NEP 表型相比,QCT 上具有 EP 表型的重度吸烟者更可能存在气流受限、预计 FEV1 更差,且类似加重发作的发生率更高。在 PFT 上无气流受限的患者中,约有 23%被归类为 EP 表型。