Axel Hauschild, University Hospital Schleswig-Holstein, Kiel; Dirk Schadendorf, University Hospital Essen, Essen; German Cancer Consortium, Heidelberg, Germany; Reinhard Dummer, University Hospital Zürich Skin Cancer Center, Zürich; Tomas Haas, Novartis AG, Basel, Switzerland; Mario Santinami, Fondazione Istituto Nazionale Tumori, Milan; Mario Mandalà, Papa Giovanni XXIII Cancer Center Hospital, Bergamo; Vanna Chiarion-Sileni, Veneto Institute of Oncology-Istituto di Ricovero e Cura a Carattere Scientifico, Padova, Italy; Victoria Atkinson, Princess Alexandra Hospital; Gallipoli Medical Research Foundation; University of Queensland, Brisbane, Queensland; Andrew Haydon, The Alfred Hospital, Melbourne, Victoria; Richard Kefford, Macquarie University; Westmead Hospital; Richard Kefford and Georgina V. Long, Melanoma Institute Australia; University of Sydney; Royal North Shore and Mater Hospitals, Sydney, New South Wales, Australia; James Larkin, Royal Marsden National Health Service Foundation Trust, London; Ruth Plummer, Freeman Hospital and Newcastle University, Newcastle upon Tyne, United Kingdom; Marta Nyakas, Oslo University Hospital, Oslo, Norway; Caroline Dutriaux, Centre Hospitalier Universitaire de Bordeaux, Hôpital Saint-André, Bordeaux; Caroline Robert, Institute Gustave Roussy, Paris; Laurent Mortier, Université de Lille, Institut National de la Santé et de la Recherche Médicale U1189, Centre Hospitalier Universitaire de sa Region Lille, Lille; Thierry Lesimple, Centre Eugène Marquis, Rennes, France; Jacob Schachter, Sheba Medical Center, Tel Hashomer; Tel Aviv University, Tel Aviv, Israel; Kohinoor Dasgupta, Novartis Healthcare, Hyderabad, India; Mark Shilkrut and Eduard Gasal, Novartis Pharmaceuticals Corporation, East Hanover, NJ; and John M. Kirkwood, UPMC Hillman Cancer Center; University of Pittsburgh, Pittsburgh, PA.
J Clin Oncol. 2018 Dec 10;36(35):3441-3449. doi: 10.1200/JCO.18.01219. Epub 2018 Oct 22.
Dabrafenib plus trametinib improved relapse-free survival (RFS) versus placebo (hazard ratio [HR], 0.47; < .001) in patients with resected V600-mutant stage III melanoma (BRF115532; COMBI-AD; ClinicalTrials.gov identifier: NCT01682083). We present an updated RFS analysis on the basis of extended study follow-up and a cure-rate model analysis to estimate the fraction of patients expected to remain relapse free long term.
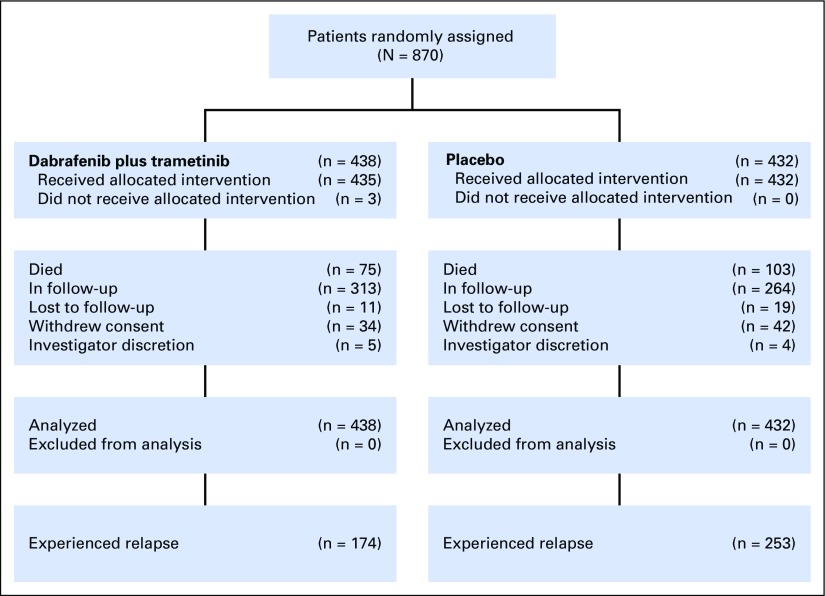
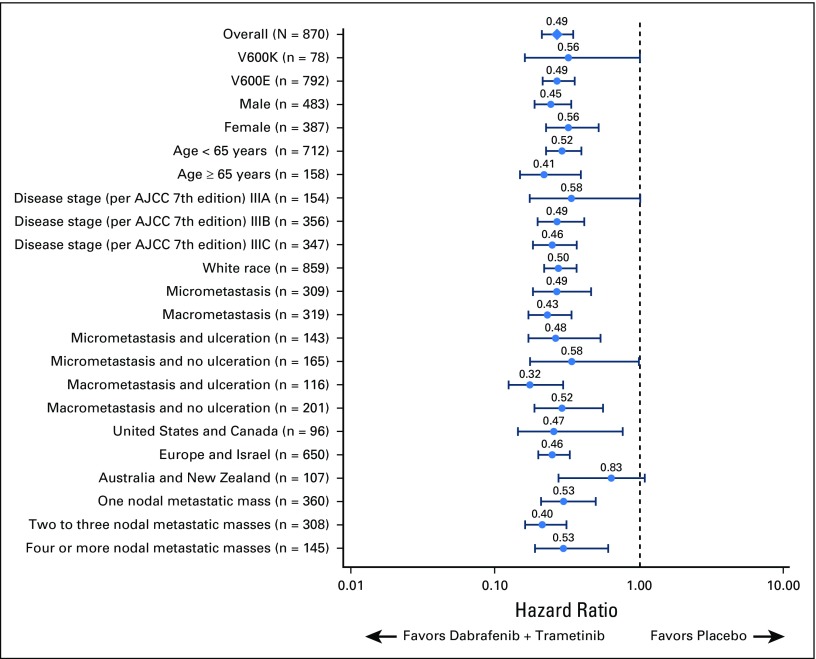
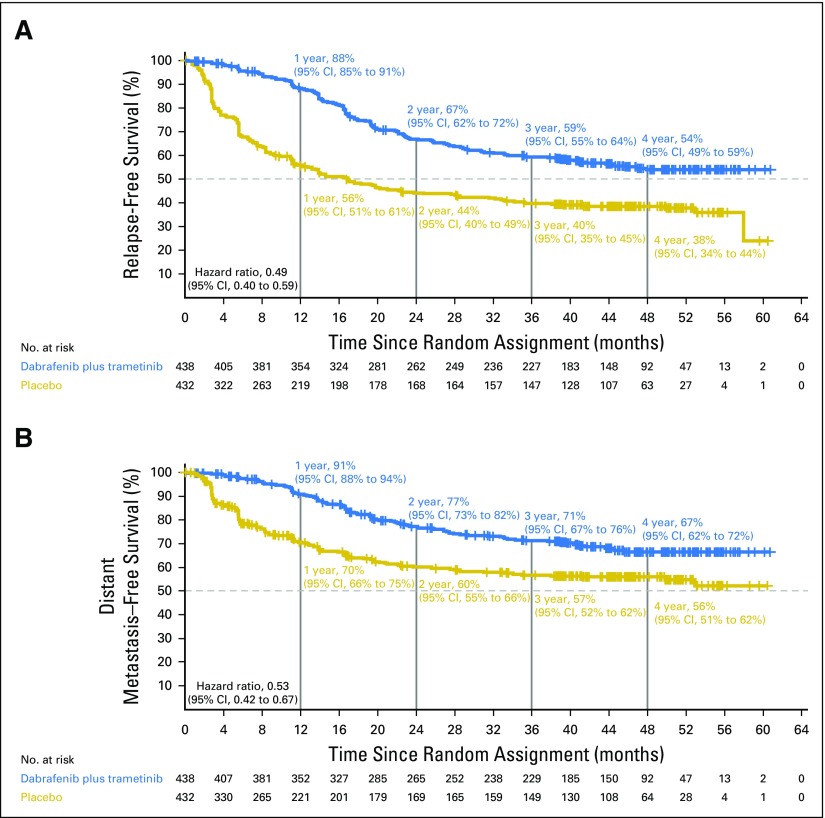
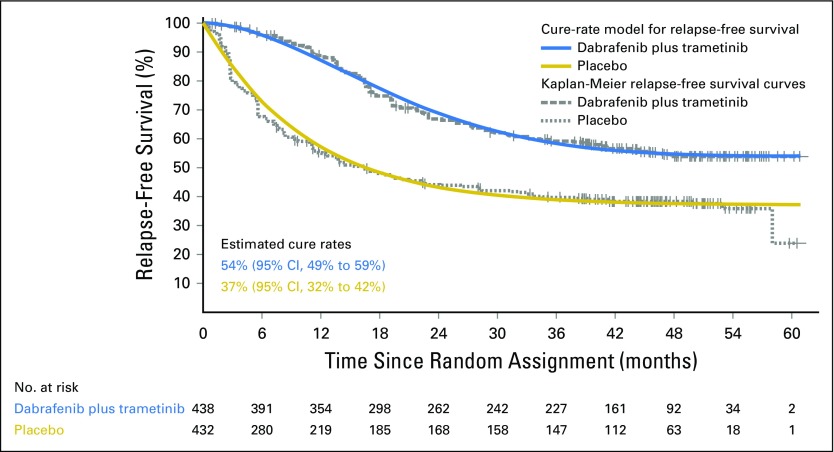
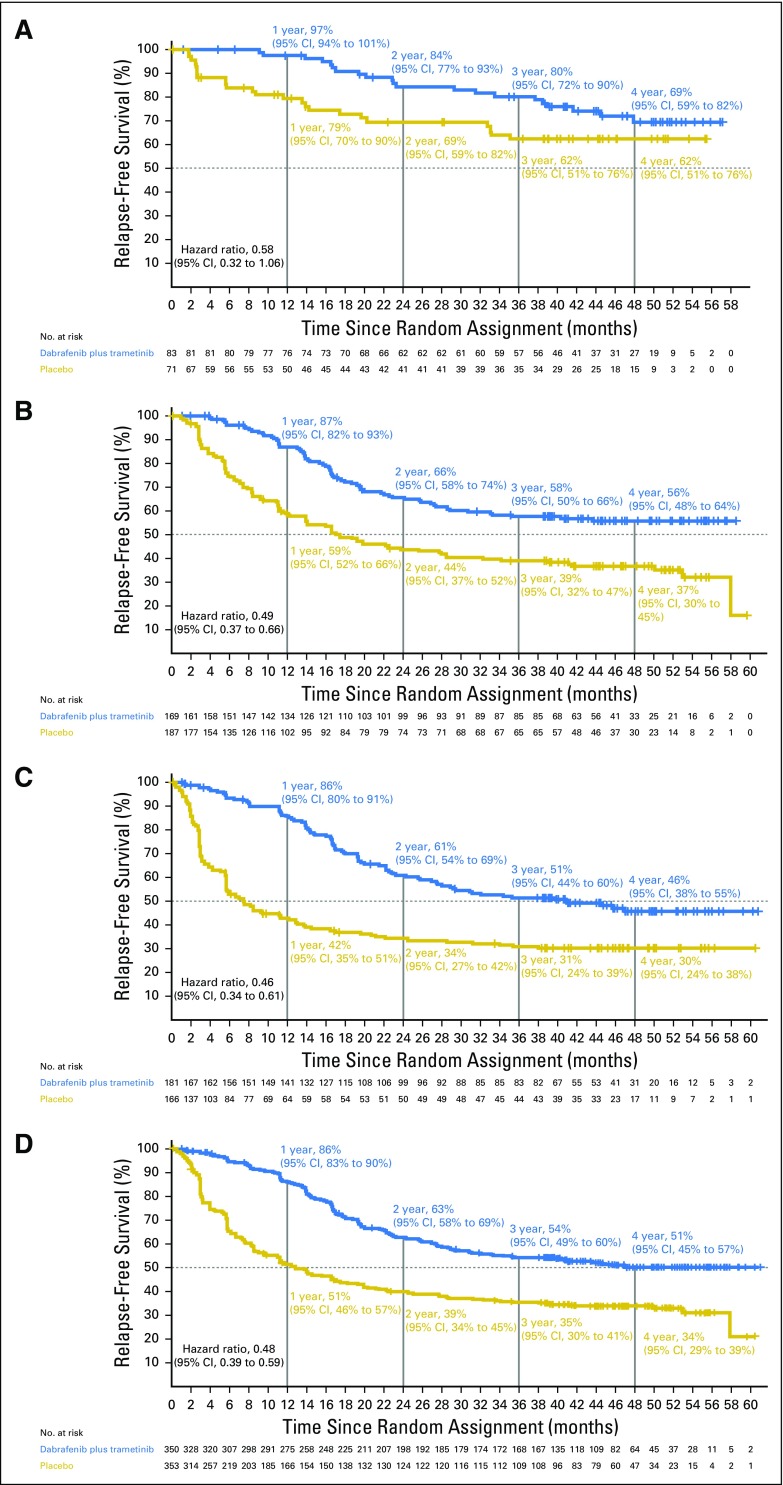
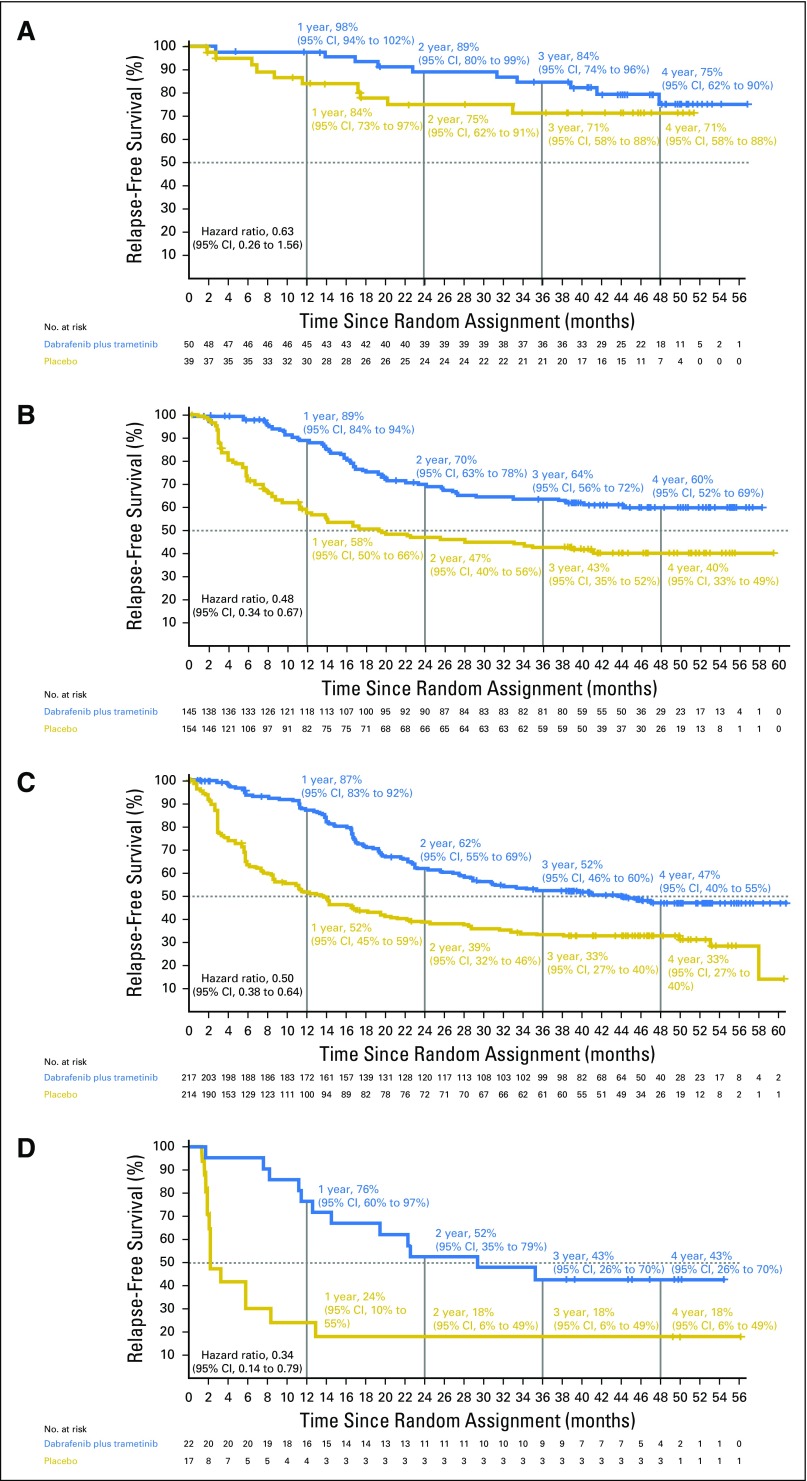
In this phase III trial, patients with resected V600-mutant stage III melanoma were randomly assigned to 12 months of adjuvant dabrafenib plus trametinib versus placebo. We report updated RFS (primary end point) and distant metastasis-free survival. RFS was also analyzed by subgroups defined by baseline disease stage (American Joint Committee on Cancer 7th and 8th editions), nodal metastatic burden, and ulceration status. The fraction of patients who remained relapse free long term was estimated using a Weibull mixture cure-rate model.
At median follow-up of 44 months (dabrafenib plus trametinib) and 42 months (placebo), 3- and 4-year RFS rates were 59% (95% CI, 55% to 64%) and 54% (95% CI, 49% to 59%) in the dabrafenib plus trametinib arm and 40% (95% CI, 35% to 45%) and 38% (95% CI, 34% to 44%) in the placebo arm, respectively (HR, 0.49; 95% CI, 0.40 to 0.59). Distant metastasis-free survival also favored dabrafenib plus trametinib (HR, 0.53; 95% CI, 0.42 to 0.67). The estimated cure rate was 54% (95% CI, 49% to 59%) in the dabrafenib plus trametinib arm compared with 37% (95% CI, 32% to 42%) in the placebo arm. Subgroup analysis of RFS demonstrated similar treatment benefit regardless of baseline factors, including disease stage, nodal metastatic burden, and ulceration.
Longer follow-up confirmed RFS benefit with dabrafenib plus trametinib. Subgroup analysis suggested that dabrafenib plus trametinib benefited patients regardless of baseline factors.
在接受手术切除的 V600 突变 III 期黑色素瘤患者中,与安慰剂相比,达拉非尼联合曲美替尼可改善无复发生存(RFS)(风险比[HR],0.47;<.001)(BRF115532;COMBI-AD;ClinicalTrials.gov 标识符:NCT01682083)。我们根据研究随访时间的延长和治愈率模型分析提供了 RFS 的更新分析结果,以估计预计长期无复发的患者比例。
在这项 III 期试验中,接受手术切除的 V600 突变 III 期黑色素瘤患者被随机分配接受 12 个月的辅助达拉非尼联合曲美替尼或安慰剂治疗。我们报告了更新的 RFS(主要终点)和远处无转移生存情况。还根据基线疾病分期(美国癌症联合委员会第 7 版和第 8 版)、淋巴结转移负担和溃疡状态对 RFS 进行了亚组分析。使用威布尔混合治愈率模型估计长期无复发的患者比例。
在中位随访 44 个月(达拉非尼联合曲美替尼)和 42 个月(安慰剂)时,达拉非尼联合曲美替尼组的 3 年和 4 年 RFS 率分别为 59%(95%CI,55%至 64%)和 54%(95%CI,49%至 59%),安慰剂组分别为 40%(95%CI,35%至 45%)和 38%(95%CI,34%至 44%)(HR,0.49;95%CI,0.40 至 0.59)。远处无转移生存也有利于达拉非尼联合曲美替尼(HR,0.53;95%CI,0.42 至 0.67)。达拉非尼联合曲美替尼组的估计治愈率为 54%(95%CI,49%至 59%),而安慰剂组为 37%(95%CI,32%至 42%)。RFS 的亚组分析表明,无论基线因素如何,包括疾病分期、淋巴结转移负担和溃疡,都观察到了类似的治疗益处。
更长时间的随访证实了达拉非尼联合曲美替尼可带来 RFS 获益。亚组分析表明,达拉非尼联合曲美替尼使患者受益,无论基线因素如何。