Centre for Advanced Reconstruction of Extremities (CARE), Sahlgrenska University Hospital/Mölndal, Mölndal, Sweden.
Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
J Spinal Cord Med. 2020 Jul;43(4):462-469. doi: 10.1080/10790268.2018.1535639. Epub 2018 Oct 23.
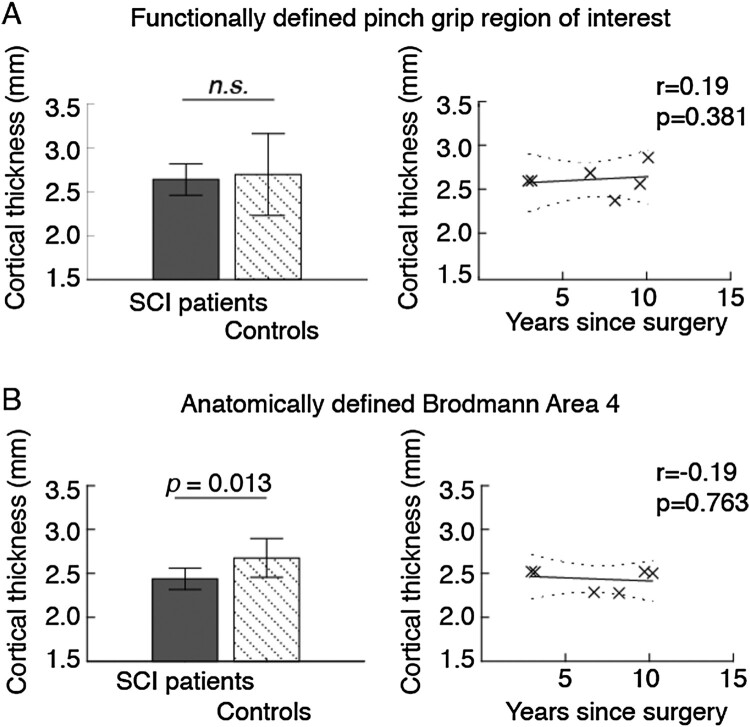
Spinal cord injury (SCI) causes atrophy of brain regions linked to motor function. We aimed to estimate cortical thickness in brain regions that control surgically restored limb movement in individuals with tetraplegia. Cross-sectional study. Sahlgrenska University hospital, Gothenburg, Sweden. Six individuals with tetraplegia who had undergone surgical restoration of grip function by surgical transfer of one elbow flexor (brachioradialis), to the paralyzed thumb flexor (flexor pollicis longus). All subjects were males, with a SCI at the C6 or C7 level, and a mean age of 40 years (range = 31-48). The average number of years elapsed since the SCI was 13 (range = 6-26). We used structural magnetic resonance imaging (MRI) to estimate the thickness of selected motor cortices and compared these measurements to those of six matched control subjects. The pinch grip control area was defined in a previous functional MRI study. Compared to controls, the cortical thickness in the functionally defined pinch grip control area was not significantly reduced (P = 0.591), and thickness showed a non-significant but positive correlation with years since surgery in the individuals with tetraplegia. In contrast, the anatomically defined primary motor cortex as a whole exhibited substantial atrophy (P = 0.013), with a weak negative correlation with years since surgery. Individuals with tetraplegia do not seem to have reduced cortical thickness in brain regions involved in control of surgically restored limb movement. However, the studied sample is very small and further studies with larger samples are required to establish these findings.
脊髓损伤(SCI)会导致与运动功能相关的大脑区域萎缩。我们旨在评估控制四肢瘫痪患者手术恢复手部运动的大脑区域的皮质厚度。 横断面研究。 瑞典哥德堡 Sahlgrenska 大学医院。 6 名四肢瘫痪患者通过手术将一只肘部屈肌(肱桡肌)转移到瘫痪的拇指屈肌(拇长屈肌)来恢复抓握功能。所有受试者均为男性,SCI 位于 C6 或 C7 水平,平均年龄为 40 岁(范围 31-48 岁)。自 SCI 以来的平均时间为 13 年(范围 6-26 年)。 我们使用结构磁共振成像(MRI)来估计选定运动皮质的厚度,并将这些测量值与 6 名匹配的对照组进行比较。之前的功能 MRI 研究定义了捏夹控制区。 与对照组相比,功能定义的捏夹控制区的皮质厚度没有明显减少(P=0.591),并且在四肢瘫痪患者中,厚度与手术以来的年数呈非显著正相关。相比之下,整个解剖定义的初级运动皮层表现出明显的萎缩(P=0.013),与手术以来的年数呈弱负相关。 四肢瘫痪患者似乎没有减少参与控制手术恢复肢体运动的大脑区域的皮质厚度。然而,研究样本非常小,需要进行更大样本量的进一步研究来确定这些发现。