Cheng Andrew L, Kaslow Abraham M, Pruetz Jay D, Lu Jimmy C, Wood John C, Detterich Jon A
Division of Pediatric Cardiology, Children's Hospital Los Angeles, 4650 Sunset Blvd., Mailstop #34, Los Angeles, CA, 90027, USA.
Keck School of Medicine, University of Southern California, Los Angeles, CA, USA.
Pediatr Cardiol. 2019 Mar;40(3):526-536. doi: 10.1007/s00246-018-2009-2. Epub 2018 Oct 23.
Patients with pulmonary atresia with intact ventricular septum and critical pulmonary stenosis (PAIVS/CPS) have wide variation in right ventricle (RV) size, systolic function, and diastolic function at birth. Establishment of antegrade pulmonary blood flow creates the potential for RV dilation from chronic pulmonary insufficiency. Future surgical decisions are based on RV size and function, largely supported by longitudinal studies of patients with Tetralogy of Fallot (TOF). Given potential differences in RV physiology and lack of similar data in PAIVS/CPS, the objective of this study was to determine differences in RV size, systolic function, and diastolic function between patients with PAIVS/CPS versus TOF.
We retrospectively collected cardiovascular magnetic resonance (CMR) data in 27 patients with PAIVS/CPS (ages 13.3 ± 8.8 years) and 78 with TOF (11.4 ± 5.4 years). RV volumes, ejection fraction (EF), regurgitant fraction, end-diastolic forward flow across the pulmonary valve, and right atrial cross-sectional area were calculated.
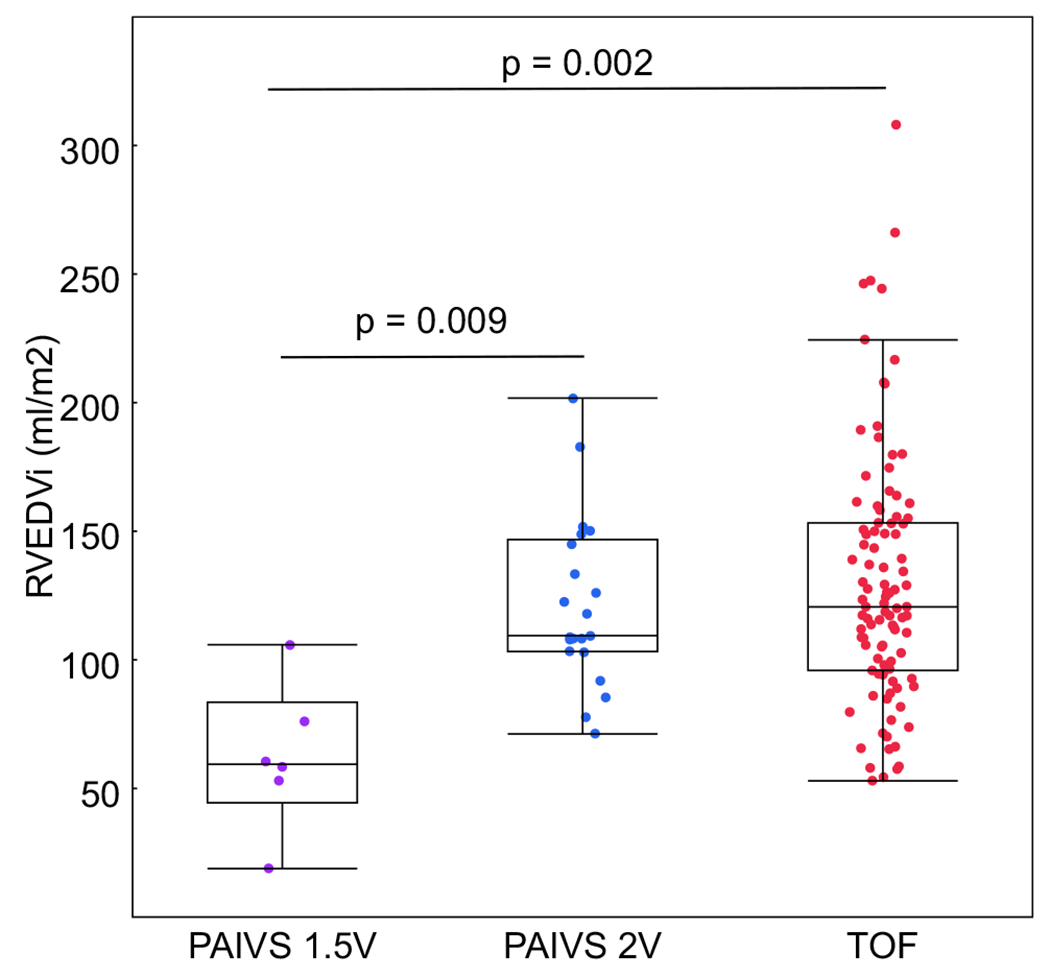
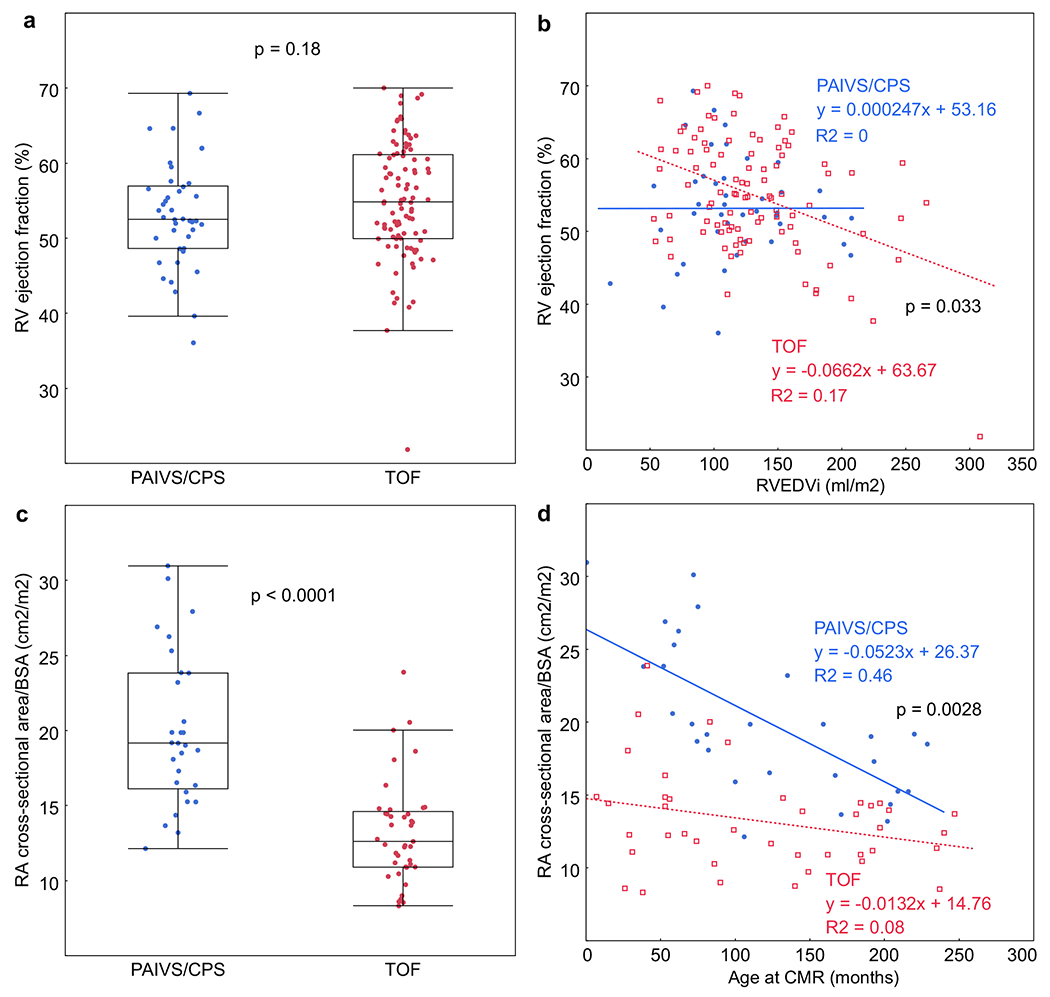
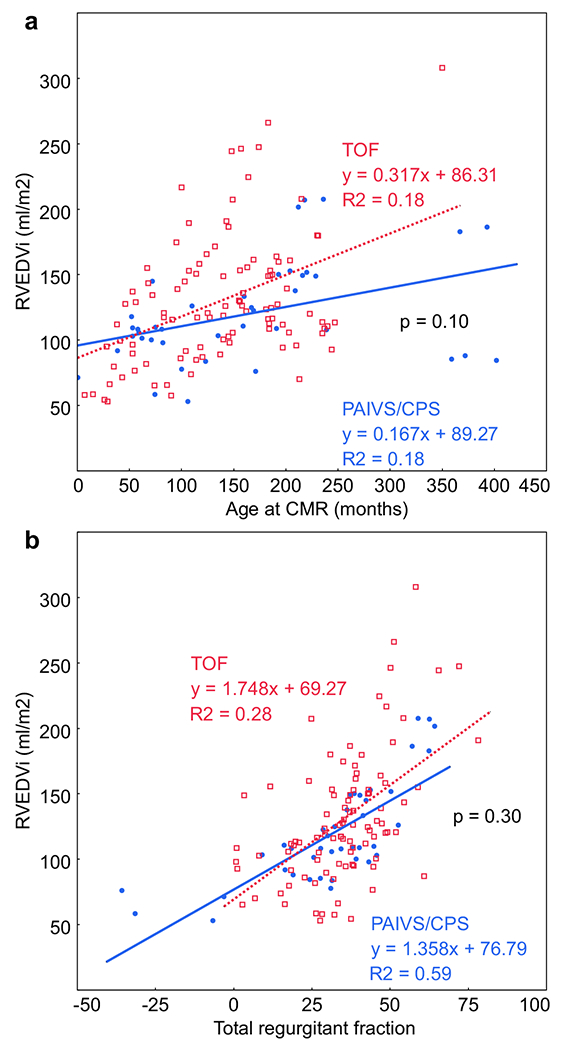
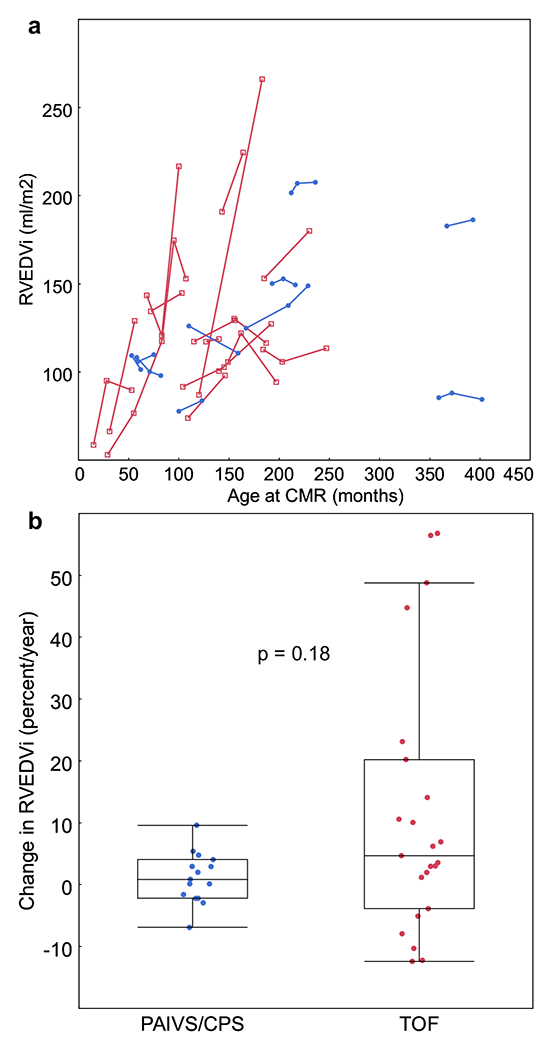
There was no difference between the groups in RV end-diastolic volume (RVEDVi), RVEF, or pulmonary regurgitation. RVEF tended to decrease in TOF when RVEDVi exceeded 164 ml/m. In PAIVS/CPS, RVEDVi less frequently reached 164 ml/m and was not associated with RVEF. There was worse RV diastolic dysfunction in PAIVS/CPS, with 1.5 times larger right atrial area and two times higher pulmonary end-diastolic forward flow (p < 0.0001).
Patients with PAIVS/CPS have similar RV size, systolic function, and pulmonary regurgitation as TOF. However, impaired RV diastolic function may limit extremes of RV dilatation and impact long-term management of PAIVS/CPS.
室间隔完整的肺动脉闭锁合并严重肺动脉狭窄(PAIVS/CPS)患者出生时右心室(RV)大小、收缩功能和舒张功能存在很大差异。建立顺行性肺血流会因慢性肺功能不全而导致右心室扩张。未来的手术决策基于右心室大小和功能,这在很大程度上得到了法洛四联症(TOF)患者纵向研究的支持。鉴于右心室生理学存在潜在差异且PAIVS/CPS缺乏类似数据,本研究的目的是确定PAIVS/CPS患者与TOF患者在右心室大小、收缩功能和舒张功能方面的差异。
我们回顾性收集了27例PAIVS/CPS患者(年龄13.3±8.8岁)和78例TOF患者(11.4±5.4岁)的心血管磁共振(CMR)数据。计算右心室容积、射血分数(EF)、反流分数、经肺动脉瓣的舒张末期正向血流以及右心房横截面积。
两组在右心室舒张末期容积(RVEDVi)、右心室射血分数(RVEF)或肺反流方面无差异。当RVEDVi超过164 ml/m时,TOF患者的RVEF往往会降低。在PAIVS/CPS中,RVEDVi较少达到164 ml/m,且与RVEF无关。PAIVS/CPS患者存在更严重的右心室舒张功能障碍,右心房面积大1.5倍,肺舒张末期正向血流高2倍(p<0.0001)。
PAIVS/CPS患者的右心室大小、收缩功能和肺反流与TOF患者相似。然而,右心室舒张功能受损可能会限制右心室扩张的程度,并影响PAIVS/CPS的长期管理。