Cruces Pablo, González-Dambrauskas Sebastián, Cristiani Federico, Martínez Javier, Henderson Ronnie, Erranz Benjamin, Díaz Franco
Pediatric Intensive Care Unit, Hospital El Carmen de Maipú, Santiago, Chile.
Centro de Investigación de Medicina Veterinaria, Escuela de Medicina Veterinaria, Facultad de Ecología y Recursos Naturales, Universidad Andres Bello, Santiago, Chile.
BMC Anesthesiol. 2018 Oct 24;18(1):151. doi: 10.1186/s12871-018-0611-8.
Positive end-expiratory pressure (PEEP) has been demonstrated to decrease ventilator-induced lung injury in patients under mechanical ventilation (MV) for acute respiratory failure. Recently, some studies have proposed some beneficial effects of PEEP in ventilated patients without lung injury. The influence of PEEP on respiratory mechanics in children is not well known. Our aim was to determine the effects on respiratory mechanics of setting PEEP at 5 cmHO in anesthetized healthy children.
Patients younger than 15 years old without history of lung injury scheduled for elective surgery gave informed consent and were enrolled in the study. After usual care for general anesthesia, patients were placed on volume controlled MV. Two sets of respiratory mechanics studies were performed using inspiratory and expiratory breath hold, with PEEP 0 and 5 cmHO. The maximum inspiratory and expiratory flow (Q and Q) as well as peak inspiratory pressure (PIP), plateau pressure (P) and total PEEP (tPEEP) were measured. Respiratory system compliance (C), inspiratory and expiratory resistances (RawI and RawE) and time constants (K and K) were calculated. Data were expressed as median and interquartile range (IQR). Wilcoxon sign test and Spearman's analysis were used. Significance was set at P < 0.05.
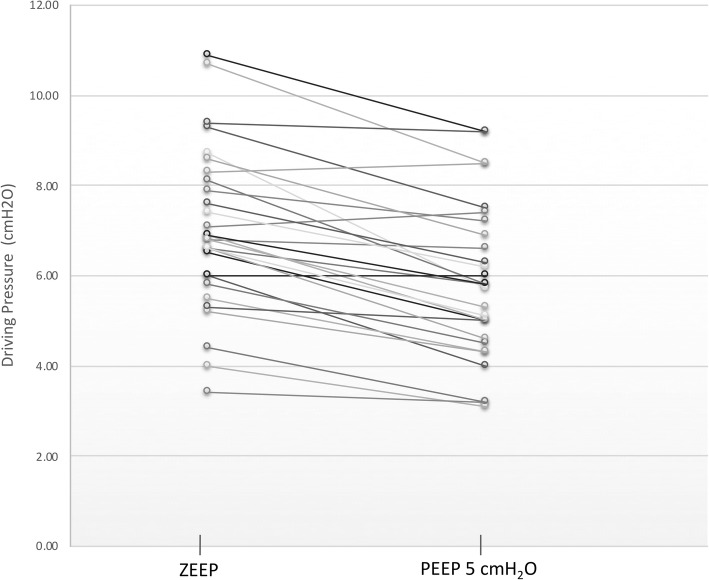
We included 30 patients, median age 39 (15-61.3) months old, 60% male. When PEEP increased, PIP increased from 12 (11,14) to 15.5 (14,18), and C increased from 0.9 (0.9,1.2) to 1.2 (0.9,1.4) mL·kg·cmHO; additionally, when PEEP increased, driving pressure decreased from 6.8 (5.9,8.1) to 5.8 (4.7,7.1) cmHO, and Q decreased from 13.8 (11.8,18.7) to 11.7 (9.1,13.5) L·min (all P < 0.01). There were no significant changes in resistance and Q.
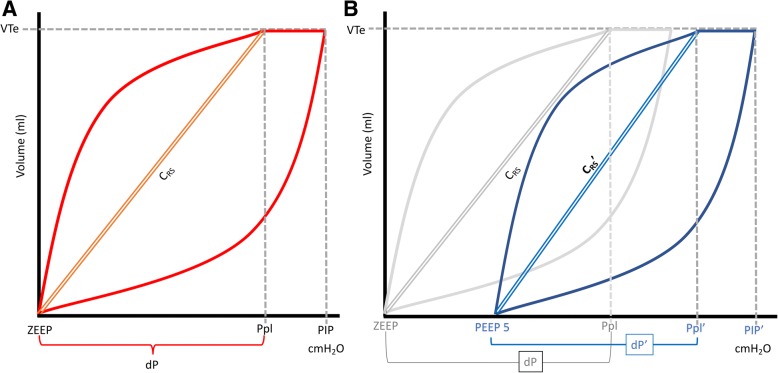
Analysis of respiratory mechanics in anesthetized healthy children shows that PEEP at 5 cmHO places the respiratory system in a better position in the P/V curve. A better understanding of lung mechanics may lead to changes in the traditional ventilatory approach, limiting injury associated with MV.
呼气末正压通气(PEEP)已被证明可减少急性呼吸衰竭机械通气(MV)患者的呼吸机诱导性肺损伤。最近,一些研究提出了PEEP对无肺损伤的机械通气患者的一些有益作用。PEEP对儿童呼吸力学的影响尚不清楚。我们的目的是确定在麻醉的健康儿童中将PEEP设置为5 cmH₂O对呼吸力学的影响。
计划进行择期手术且无肺损伤病史的15岁以下患者签署知情同意书并纳入研究。在进行常规全身麻醉护理后,患者接受容量控制通气。使用吸气和呼气屏气法进行两组呼吸力学研究,PEEP分别为0和5 cmH₂O。测量最大吸气和呼气流量(Qₐ和Qₑ)以及吸气峰压(PIP)、平台压(Pplat)和总PEEP(tPEEP)。计算呼吸系统顺应性(Crs)、吸气和呼气阻力(RawI和RawE)以及时间常数(τI和τE)。数据以中位数和四分位间距(IQR)表示。采用Wilcoxon符号检验和Spearman分析。显著性设定为P < 0.05。
我们纳入了30例患者,中位年龄39(15 - 61.3)个月,60%为男性。当PEEP增加时,PIP从12(11, 14)增加至15.5(14, 18),Crs从0.9(0.9, 1.2)增加至1.2(0.9, 1.4)mL·kg⁻¹·cmH₂O⁻¹;此外,当PEEP增加时,驱动压从6.8(5.9, 8.1)降至5.8(4.7, 7.1)cmH₂O,Qₐ从13.8(11.8, 18.7)降至11.7(9.1, 13.5)L·min(所有P < 0.01)。阻力和Qₑ无显著变化。
对麻醉的健康儿童呼吸力学的分析表明,5 cmH₂O的PEEP使呼吸系统在压力 - 容积(P/V)曲线中处于更佳位置。更好地理解肺力学可能会导致传统通气方法的改变,限制与MV相关的损伤。