Bein Thomas, Grasso Salvatore, Moerer Onnen, Quintel Michael, Guerin Claude, Deja Maria, Brondani Anita, Mehta Sangeeta
Department of Anesthesia, Operative Intensive Care, University Hospital Regensburg, 93042, Regensburg, Germany.
Dipartimento dell'Emergenza e Trapianti d'Organo (DETO), Sezione di Anestesiologia e Rianimazione, Università degli Studi di Bari "Aldo Moro", Bari, Italy.
Intensive Care Med. 2016 May;42(5):699-711. doi: 10.1007/s00134-016-4325-4. Epub 2016 Apr 4.
Severe ARDS is often associated with refractory hypoxemia, and early identification and treatment of hypoxemia is mandatory. For the management of severe ARDS ventilator settings, positioning therapy, infection control, and supportive measures are essential to improve survival.
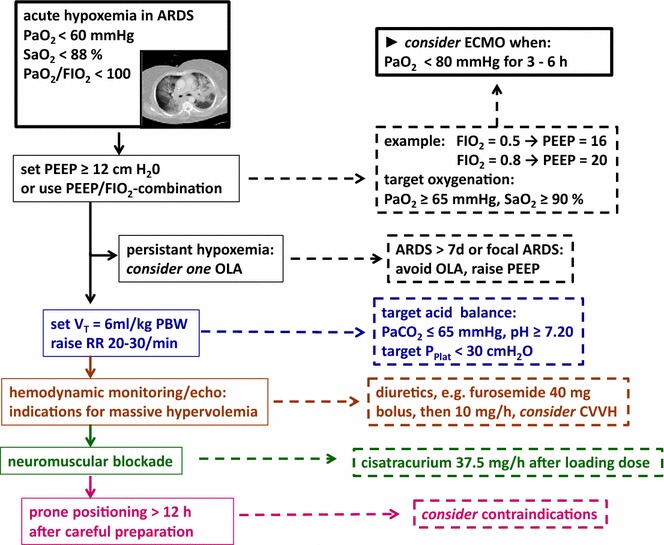
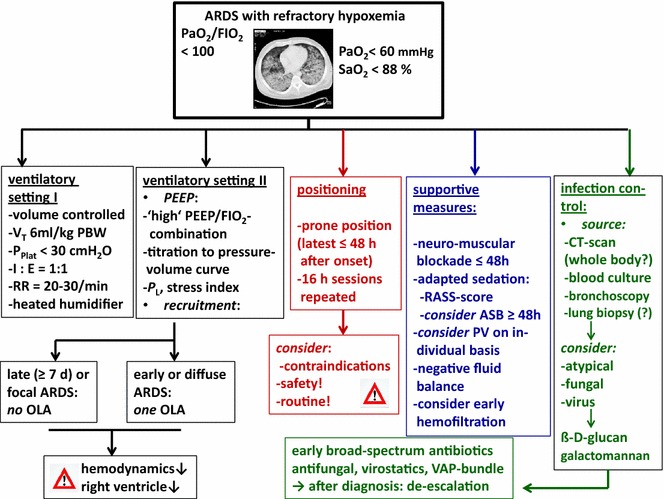
A precise definition of life-threating hypoxemia is not identified. Typical clinical determinations are: arterial partial pressure of oxygen < 60 mmHg and/or arterial oxygenation < 88 % and/or the ratio of PaO2/FIO2 < 100. For mechanical ventilation specific settings are recommended: limitation of tidal volume (6 ml/kg predicted body weight), adequate high PEEP (>12 cmH2O), a recruitment manoeuvre in special situations, and a 'balanced' respiratory rate (20-30/min). Individual bedside methods to guide PEEP/recruitment (e.g., transpulmonary pressure) are not (yet) available. Prone positioning [early (≤ 48 hrs after onset of severe ARDS) and prolonged (repetition of 16-hr-sessions)] improves survival. An advanced infection management/control includes early diagnosis of bacterial, atypical, viral and fungal specimen (blood culture, bronchoalveolar lavage), and of infection sources by CT scan, followed by administration of broad-spectrum anti-infectives. Neuromuscular blockage (Cisatracurium ≤ 48 hrs after onset of ARDS), as well as an adequate sedation strategy (score guided) is an important supportive therapy. A negative fluid balance is associated with improved lung function and the use of hemofiltration might be indicated for specific indications.
A specific standard of care is required for the management of severe ARDS with refractory hypoxemia.
重症急性呼吸窘迫综合征(ARDS)常伴有难治性低氧血症,早期识别和治疗低氧血症至关重要。对于重症ARDS的管理,呼吸机设置、体位治疗、感染控制和支持措施对于提高生存率至关重要。
尚未确定危及生命的低氧血症的精确定义。典型的临床判定标准为:动脉血氧分压<60 mmHg和/或动脉氧合<88%和/或动脉血氧分压与吸入氧分数值之比(PaO2/FIO2)<100。对于机械通气,推荐采用特定设置:限制潮气量(6 ml/kg预计体重)、足够高的呼气末正压(PEEP,>12 cmH2O)、特殊情况下的肺复张手法以及“平衡”的呼吸频率(20 - 30次/分钟)。尚无(目前还没有)用于指导PEEP/肺复张的个体化床旁方法(例如,跨肺压)。俯卧位通气[早期(重症ARDS发病后≤48小时)和延长(重复16小时疗程)]可提高生存率。先进的感染管理/控制包括通过血培养、支气管肺泡灌洗等对细菌、非典型病原体、病毒和真菌标本以及感染源进行早期诊断,随后给予广谱抗感染药物。神经肌肉阻滞(ARDS发病后≤48小时使用顺式阿曲库铵)以及适当的镇静策略(评分指导)是重要的支持治疗。负液体平衡与肺功能改善相关,对于特定指征可能需要使用血液滤过。
对于伴有难治性低氧血症的重症ARDS的管理,需要特定的护理标准。