Ricci Jean-Etienne, Kalmanovich Eran, Robert Christelle, Chevallier Thierry, Aguilhon Sylvain, Solecki Kamila, Akodad Mariama, Cornillet Luc, Soullier Camille, Cayla Guillaume, Lattuca Benoit, Roubille François
Department of Cardiology, Nîmes University Hospital, University of Montpellier, Nîmes, France.
Department of Cardiology, Montpellier University Hospital, 34295, Montpellier Cedex 5, France.
Contemp Clin Trials Commun. 2018 Aug 9;12:103-108. doi: 10.1016/j.conctc.2018.07.006. eCollection 2018 Dec.
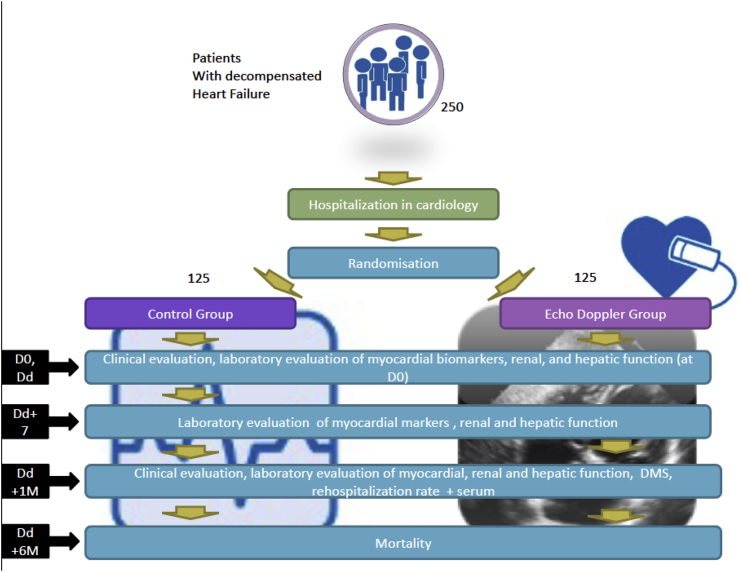
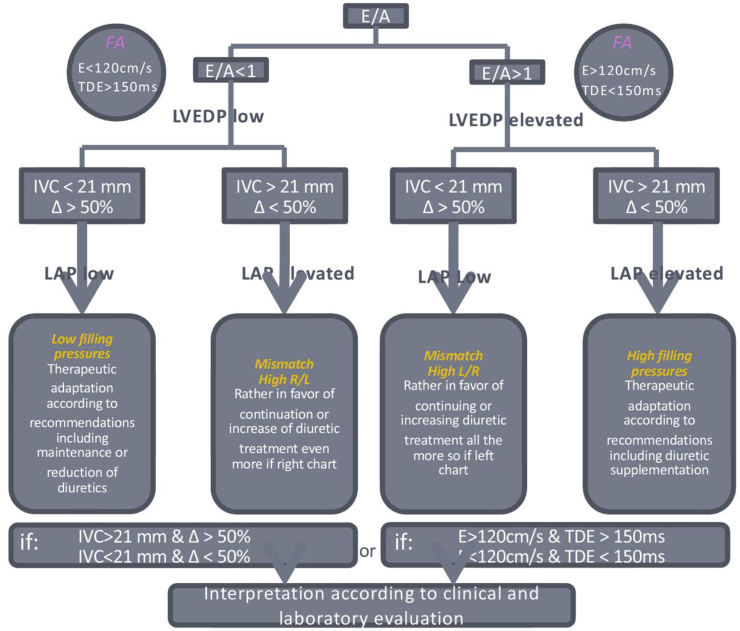
There are currently one million heart failure (HF) patients in France and the rate is progressively increases due to population aging. Acute decompensation of HF is the leading cause of hospitalization in people over 65 years of age with a 25% re-hospitalization rate in the first month. Expenses related to the management of HF in France in 2013 amounted to more than one billion euros, of which 65% were for hospitalizations alone. The management of acute decompensation is a challenge, due to the complexity of clinical and laboratory evaluation leading to therapeutic errors, which in turn leads to longer hospitalization, high early re-hospitalization and complications. Therapeutic adjustment, especially diuretic, in the acute phase (during hospitalization) affects early re-hospitalization rates (within 30 days). These adjustments can be based on clinical estimation and laboratory parameters, but echocardiography has been shown to be superior in estimating filling pressures (FP) compared to clinical and laboratory parameters. We hypothesize that a simple daily bedside echocardiographic assessment could provide a reproducible estimation of FP with an evaluation of mitral inflow and the inferior vena cava (IVC). This could allow a more reliable estimate of the true blood volume of the patient and thus lead to a more suitable therapeutic adjustment. This in turn should lead to a decrease in early re-admission rate (primary endpoint) and potentially decrease six-month mortality and rate of complications.
目前法国有100万心力衰竭(HF)患者,且由于人口老龄化,这一数字正逐步上升。HF急性失代偿是65岁以上人群住院的主要原因,首月再住院率达25%。2013年法国HF治疗费用超过10亿欧元,其中仅住院费用就占65%。急性失代偿的治疗颇具挑战,因为临床和实验室评估复杂,易导致治疗失误,进而造成住院时间延长、早期再住院率高及并发症。急性期(住院期间)的治疗调整,尤其是利尿剂的调整,会影响早期再住院率(30天内)。这些调整可基于临床评估和实验室参数,但与临床及实验室参数相比,超声心动图在评估充盈压(FP)方面更具优势。我们推测,每日一次简单的床边超声心动图评估,通过评估二尖瓣血流和下腔静脉(IVC),可对FP进行可重复的评估。这能够更可靠地估计患者的实际血容量,从而实现更合适的治疗调整。这反过来应能降低早期再入院率(主要终点),并可能降低六个月死亡率及并发症发生率。