Department of Radiotherapy and Special Oncology, Medical School Hannover, Carl-Neuberg-Str. 1, 30625, Hannover, Germany.
Radiat Oncol. 2018 Nov 3;13(1):213. doi: 10.1186/s13014-018-1156-1.
To determine the prognostic impact of comorbidity and age in medically inoperable early-stage non-small cell lung cancer (NSCLC) treated with stereotactic body radiotherapy (SBRT) using the age-adjusted Charlson Comorbidity Index (aCCI).
Between November 2008 and January 2015, 196 consecutive patients with medically inoperable NSCLC were treated with SBRT at a single institution. The prescribed isocenter dose was either 60.0 Gray (Gy) in six fractions for central lung cancer or 56.25 Gy in three fractions for peripheral lung cancer. Baseline comorbidities were retrospectively retrieved according to available outclinic medical records as well as the hospital information system. The aCCI was scored for each patient and subjected according to outcome and toxicity as well as all of the single items of the aCCI and other clinical parameters using univariate and multivariate analysis.
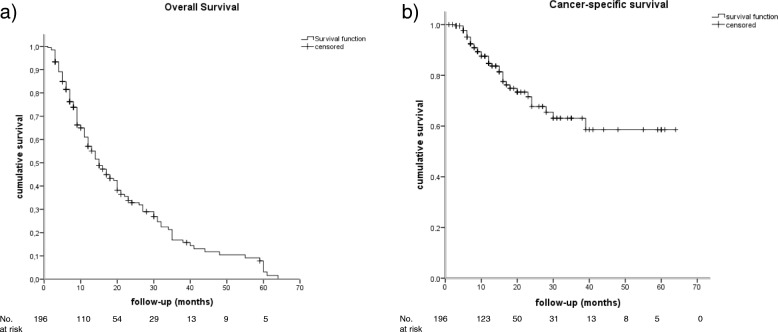
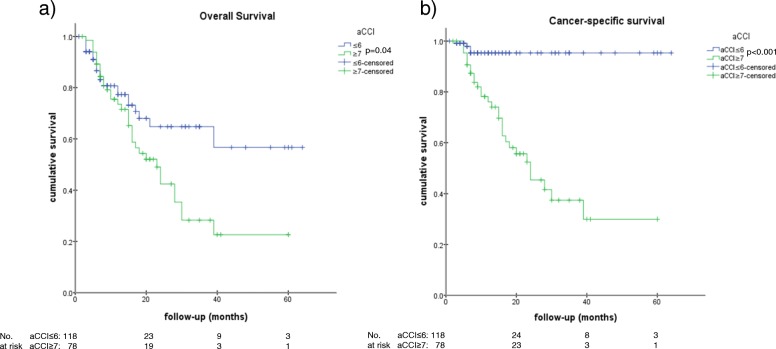
Thirty-one point 6 % (62/196) of patients were deceased, of whom 17.3% (34/196) died due to lung cancer and 14.3% (28/196) due to comorbidities. The median overall survival (OS) was 15.0 months (95% CI [11.9-18.1]), whereas the median cancer-specific survival (CSS) was not reached. An aCCI ≥7 compared with an aCCI ≤6 was significantly associated with an increased risk of death (HR 1.79, 95% CI [1.02-2.80], p = 0.04) and cancer-specific death (HR 9.26, 95% CI [4.83-24.39], p < 0.001), respectively. Neither OS nor CCS were significantly associated with age, sex, side (left vs. right), lobe, localization (central vs. peripheral), packyears, TNM, or any item of the aCCI. Considering the 14.3% (28/196) of deceased patients who died due to comorbidities, aCCI ≥9 was significantly associated with non-cancer-related death (HR 3.12, 95% CI [1.22-8.33], p = 0.02). The observed cumulative rate of radiation pneumonitis (RP) ≥2 was 12.7% (25/196). The aCCI had no statistical association with RP.
Advanced age and numerous comorbidities characterizing this patient population were successfully assessed using the aCCI in terms of survival. Therefore, we recommend that age and comorbidity be indexed using the aCCI as a simple scoring system for all patients treated with SBRT for lung cancer.
使用年龄调整 Charlson 合并症指数(aCCI)来确定不能手术的早期非小细胞肺癌(NSCLC)患者接受立体定向体放射治疗(SBRT)后的合并症和年龄的预后影响。
在 2008 年 11 月至 2015 年 1 月期间,196 名患有不能手术的 NSCLC 的患者在一家机构接受 SBRT 治疗。中央型肺癌的推荐等中心点剂量为 60.0 戈瑞(Gy)分 6 次,周围型肺癌为 56.25 Gy 分 3 次。根据可用的门诊病历和医院信息系统,回顾性地获取基线合并症。为每位患者评分 aCCI,并根据结果和毒性以及 aCCI 的所有单项和其他临床参数进行单变量和多变量分析。
31.6%(62/196)的患者死亡,其中 17.3%(34/196)死于肺癌,14.3%(28/196)死于合并症。中位总生存期(OS)为 15.0 个月(95%CI [11.9-18.1]),而中位癌症特异性生存期(CSS)尚未达到。aCCI≥7 与死亡风险增加显著相关(HR 1.79,95%CI [1.02-2.80],p=0.04)和癌症特异性死亡(HR 9.26,95%CI [4.83-24.39],p<0.001),分别。OS 和 CSS 均与年龄、性别、侧(左与右)、叶、定位(中央与外周)、吸烟包年数、TNM 或 aCCI 的任何项目均无显著相关性。考虑到 14.3%(28/196)因合并症而死亡的患者,aCCI≥9 与非癌症相关死亡显著相关(HR 3.12,95%CI [1.22-8.33],p=0.02)。≥2 级放射性肺炎(RP)的观察累积发生率为 12.7%(25/196)。aCCI 与 RP 无统计学关联。
使用 aCCI 成功评估了该患者人群的生存情况,年龄和合并症的特征。因此,我们建议在对接受 SBRT 治疗的肺癌患者进行评分时,使用 aCCI 作为年龄和合并症的简单评分系统。