National Amyloidosis Centre, University College London, London, UK.
Medical Department V, Amyloidosis Centre, University Hospital Heidelberg, Heidelberg, Germany.
Blood Cancer J. 2018 Nov 5;8(11):101. doi: 10.1038/s41408-018-0137-9.
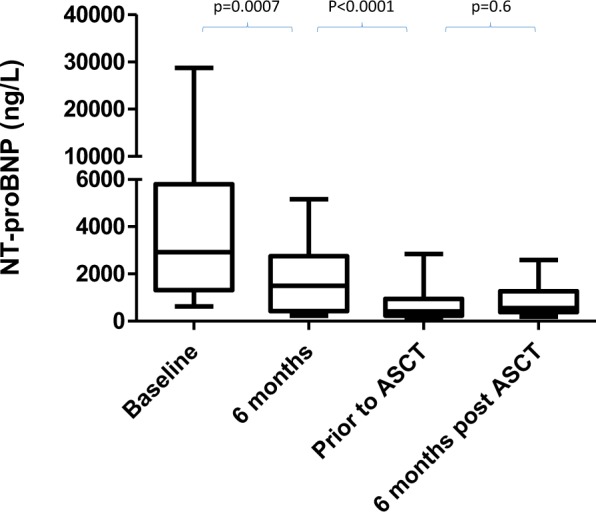
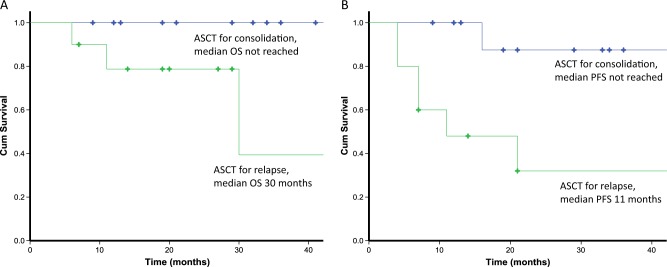
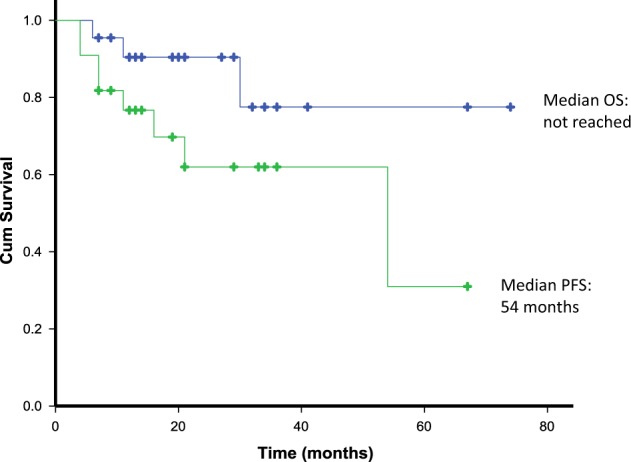
High-dose melphalan with autologous stem cell transplantation (ASCT) can induce durable haematological and organ responses in systemic AL amyloidosis (AL). Stringent selection criteria have improved safety of ASCT in AL but most patients are transplant-ineligible. We report our experience of deferred ASCT in AL patients who were transplant-ineligible at presentation but had improvements in organ function after induction chemotherapy, enabling them to undergo ASCT. Twenty-two AL patients underwent deferred ASCT from 2011 to 2017. All had serial organ function and clonal response assessment. Organ involvement and responses were defined by amyloidosis consensus criteria. All patients were transplant-ineligible at presentation, predominantly due to advanced cardiac involvement. All received bortezomib-based therapy, with 100% haematologic response (86% complete response (CR)/very good partial response (VGPR)), enabling reversal of ASCT exclusion criteria. Patients underwent deferred ASCT for haematologic progression (45%) or consolidation (55%). There was no transplant-related mortality. Haematologic responses post-ASCT: CR 50%, VGPR 27%, PR 18%, non-response 5%. In all, 85.7% achieved cardiac responses. Median overall survival (OS) was not reached. Median progression-free survival (PFS) was 54 months. This selected cohort achieved excellent haematologic responses, organ responses, PFS and OS with deferred ASCT. If larger studies confirm these findings, this may widen the applicability of ASCT in AL.
大剂量美法仑联合自体干细胞移植(ASCT)可诱导系统性轻链淀粉样变性(AL)患者持久的血液学和器官反应。严格的选择标准提高了 ASCT 在 AL 中的安全性,但大多数患者不适合进行移植。我们报告了 22 例在初诊时不适合进行 ASCT 但在诱导化疗后器官功能改善的 AL 患者接受延迟 ASCT 的经验,使他们能够进行 ASCT。2011 年至 2017 年期间,22 例 AL 患者接受了延迟 ASCT。所有患者均进行了连续的器官功能和克隆反应评估。器官受累和反应通过淀粉样变性共识标准定义。所有患者在初诊时均不适合进行移植,主要是由于心脏受累进展。所有患者均接受硼替佐米为基础的治疗,血液学反应率为 100%(86%完全缓解(CR)/非常好的部分缓解(VGPR)),使 ASCT 排除标准得以逆转。患者因血液学进展(45%)或巩固(55%)而接受延迟 ASCT。无移植相关死亡。ASCT 后的血液学反应:CR 50%,VGPR 27%,PR 18%,无反应 5%。所有患者均达到心脏反应。总生存(OS)未达到。无进展生存(PFS)为 54 个月。该选择队列通过延迟 ASCT 获得了极好的血液学反应、器官反应、PFS 和 OS。如果更大规模的研究证实了这些发现,这可能会扩大 ASCT 在 AL 中的适用性。