Department of Psychology, Division of Clinical Psychology and Psychotherapy, Philipps University Marburg, Gutenbergstr. 18, 35032, Marburg, Germany.
DRK Schmerz-Zentrum, Auf der Steig 16, 55131, Mainz, Germany.
BMC Public Health. 2018 Nov 7;18(1):1239. doi: 10.1186/s12889-018-6135-9.
A task force of the International Association for the Study of Pain (IASP) has developed a classification of chronic pain for the ICD-11 consisting of seven major categories. The objective was to test whether the proposed categories were exhaustive and mutually exclusive. In addition, the perceived utility of the diagnoses and the raters' subjective diagnostic certainty were to be assessed.
Five independent pain centers in three continents coded 507 consecutive patients. The raters received the definitions for the main diagnostic categories of the proposed classification and were asked to allocate diagnostic categories to each patient. In addition, they were asked to indicate how useful they judged the diagnosis to be from 0 (not at all) to 3 (completely) and how confident they were in their category allocation.
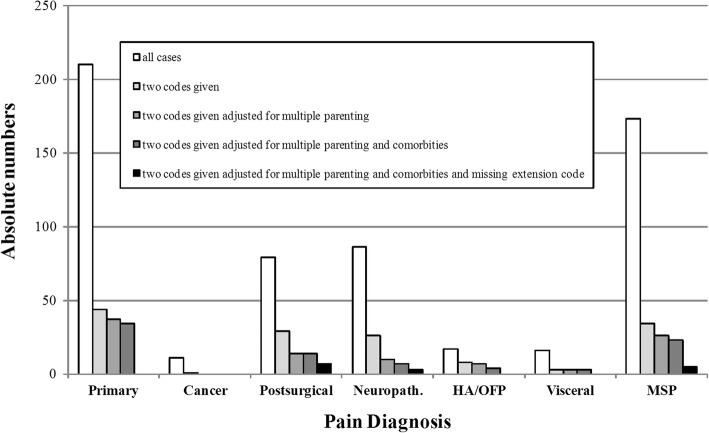
The two largest groups of patients were coded as either chronic primary pain or chronic secondary musculoskeletal pain. Of the 507 patients coded, 3.0% had chronic pain not fitting any of the proposed categories (97% exhaustiveness), 20.1% received more than one diagnosis. After adjusting for double coding due to technical reasons, 2.0% of cases remained (98% uniqueness). The mean perceived utility was 1.9 ± 1.0, the mean diagnostic confidence was 2.0 ± 1.0.
The categories proved exhaustive with few cases being classified as unspecified chronic pain, and they showed themselves to be mutually exclusive. The categories were regarded as useful with particularly high ratings for the newly introduced categories (chronic cancer-related pain among others). The confidence in allocating the diagnoses was good although no training regarding the ICD-11 categories had been possible at this stage of the development.
国际疼痛研究协会(IASP)的一个工作组为 ICD-11 制定了一个包含七个主要类别的慢性疼痛分类。目的是检验所提出的类别是否完备且互斥。此外,还评估了诊断的感知效用和评估者的主观诊断确定性。
三个大陆的五个独立疼痛中心对 507 例连续患者进行了编码。评估者收到了拟议分类的主要诊断类别的定义,并被要求将诊断类别分配给每个患者。此外,他们还被要求从 0(完全没有)到 3(完全)评估他们认为诊断的有用程度,并对他们的分类分配的信心进行评估。
最大的两组患者被编码为慢性原发性疼痛或慢性继发性肌肉骨骼疼痛。在编码的 507 例患者中,3.0%的患者患有不符合任何拟议类别的慢性疼痛(97%完备性),20.1%的患者接受了多个诊断。在调整了由于技术原因导致的双重编码后,仍有 2.0%的病例(98%的独特性)。感知有用性的平均值为 1.9±1.0,诊断置信度的平均值为 2.0±1.0。
这些类别被证明是完备的,很少有病例被归类为未指定的慢性疼痛,并且它们是互斥的。这些类别被认为是有用的,特别是对于新引入的类别(如慢性癌症相关疼痛),评分非常高。分配诊断的信心很好,尽管在 ICD-11 类别的这个开发阶段还不可能进行任何培训。