Department of Neurology, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts, United States of America.
Departments of Radiology, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts, United States of America.
PLoS One. 2018 Nov 8;13(11):e0206939. doi: 10.1371/journal.pone.0206939. eCollection 2018.
Cerebral atrophy is common in multiple sclerosis (MS) and selectively involves gray matter (GM). Several fully automated methods are available to measure whole brain and regional deep GM (DGM) atrophy from MRI.
To assess the sensitivity of fully automated MRI segmentation pipelines in detecting brain atrophy in patients with relapsing-remitting (RR) MS and normal controls (NC) over five years.
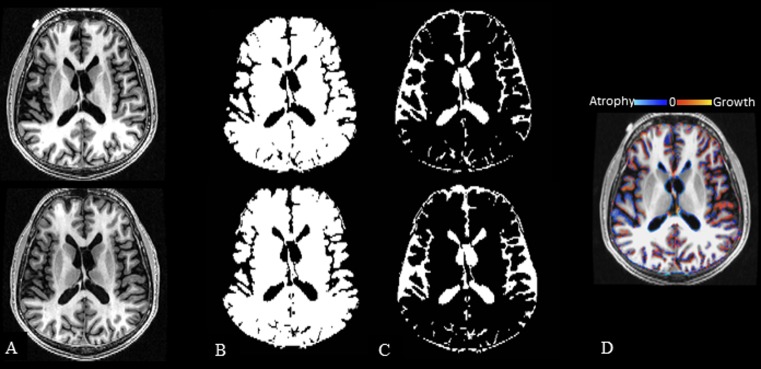
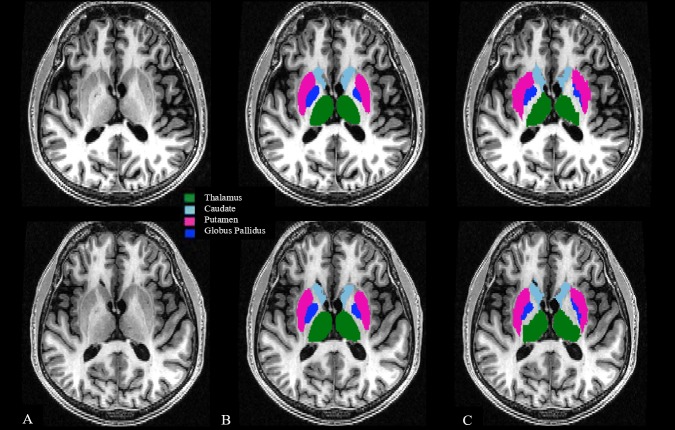
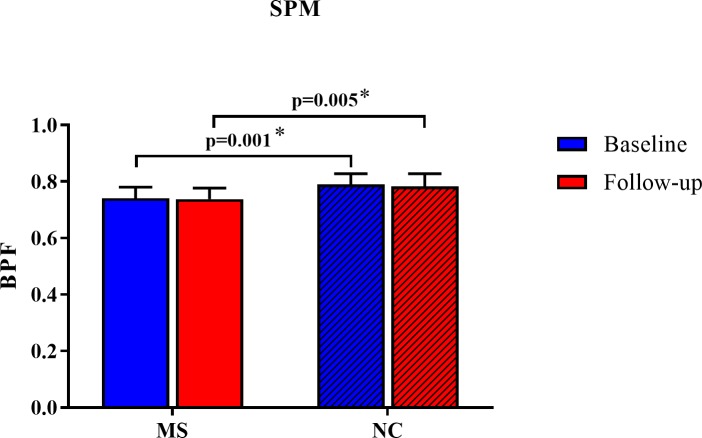
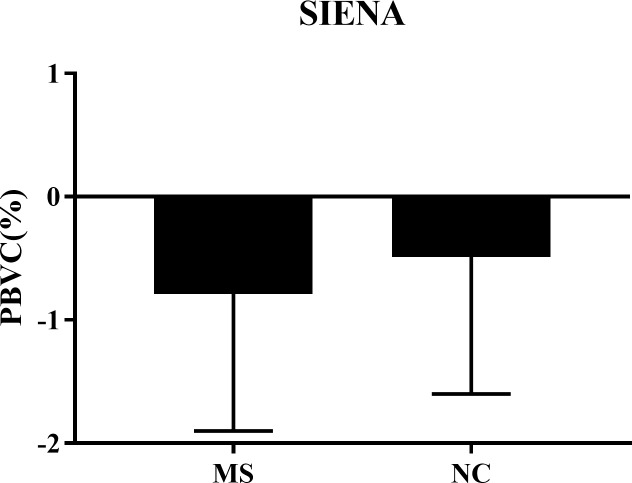
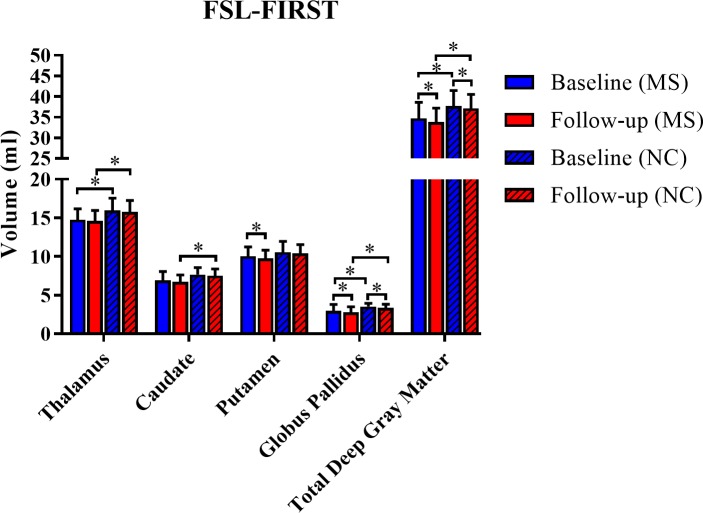
Consistent 3D T1-weighted sequences were performed on a 3T GE unit in 16 mildly disabled patients with RRMS and 16 age-matched NC at baseline and five years. All patients received disease-modifying immunotherapy on-study. Images were applied to two pipelines to assess whole brain atrophy [brain parenchymal fraction (BPF) from SPM12; percentage brain volume change (PBVC) from SIENA] and two other pipelines (FSL-FIRST; FreeSurfer) to assess DGM atrophy (thalamus, caudate, globus pallidus, putamen). MRI change was compared by two sample t-tests. Expanded Disability Status Scale (EDSS) and timed 25-foot walk (T25FW) change was compared by repeated measures proportional odds models.
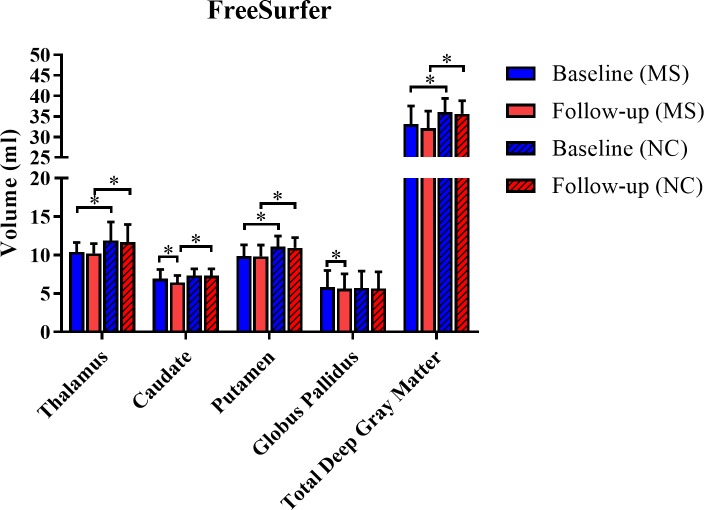
Using FreeSurfer, the MS group had a ~10-fold acceleration in on-study volume loss than NC in the caudate (mean decrease 0.51 vs. 0.05 ml, p = 0.022). In contrast, caudate atrophy was not detected by FSL-FIRST (mean decrease 0.21 vs. 0.12 ml, p = 0.53). None of the other pipelines showed any difference in volume loss between groups, for whole brain or regional DGM atrophy (all p>0.38). The MS group showed on-study stability on EDSS (p = 0.47) but slight worsening of T25FW (p = 0.054).
In this real-world cohort of mildly disabled treated patients with RRMS, we identified ongoing atrophy of the caudate nucleus over five years, despite the lack of any significant whole brain atrophy, compared to healthy controls. The detectability of caudate atrophy was dependent on the MRI segmentation pipeline employed. These findings underscore the increased sensitivity gained when assessing DGM atrophy in monitoring MS.
脑萎缩在多发性硬化症(MS)中很常见,并且选择性地涉及灰质(GM)。有几种完全自动化的方法可从 MRI 测量全脑和区域深部 GM(DGM)萎缩。
评估完全自动化的 MRI 分割管道在五年内检测复发缓解型(RR)MS 患者和正常对照(NC)的脑萎缩的敏感性。
在基线和五年时,在 3T GE 单元上对 16 名轻度残疾 RRMS 患者和 16 名年龄匹配的 NC 进行了一致的 3D T1 加权序列。所有患者均在研究期间接受了疾病修正免疫疗法。将图像应用于两个管道以评估全脑萎缩[来自 SPM12 的脑实质分数(BPF);来自 SIENA 的脑容量变化百分比(PBVC)]和另外两个管道(FSL-FIRST;FreeSurfer)以评估 DGM 萎缩(丘脑,尾状核,苍白球,壳核)。通过双样本 t 检验比较 MRI 变化。通过重复测量比例优势模型比较扩展残疾状况量表(EDSS)和 25 英尺步行计时(T25FW)变化。
使用 FreeSurfer,MS 组在研究过程中的体积损失速度比 NC 快约 10 倍在尾状核中(平均减少 0.51 与 0.05 ml,p = 0.022)。相比之下,FSL-FIRST 未检测到尾状核萎缩(平均减少 0.21 与 0.12 ml,p = 0.53)。在全脑或区域 DGM 萎缩方面,没有其他管道显示组间任何体积损失差异(均 p>0.38)。MS 组在 EDSS 上显示研究期间的稳定性(p = 0.47),但 T25FW 略有恶化(p = 0.054)。
在这项针对接受治疗的轻度残疾 RRMS 患者的真实世界队列研究中,与健康对照相比,我们发现尽管没有明显的全脑萎缩,但在五年内仍存在尾状核持续萎缩。尾状核萎缩的可检测性取决于所使用的 MRI 分割管道。这些发现强调了在监测 MS 时评估 DGM 萎缩所获得的更高敏感性。