Center for Vaccines and Immunity, Nationwide Children's Hospital and The Ohio State University College of Medicine, Columbus.
Biostatistics Core, The Research Institute at Nationwide Children's Hospital, Nationwide Children's Hospital and The Ohio State University College of Medicine, Columbus.
J Infect Dis. 2019 Apr 8;219(8):1207-1215. doi: 10.1093/infdis/jiy655.
The association between respiratory syncytial virus (RSV) loads and clinical outcomes in children remains to be defined. In most studies, viral loads (VL) were evaluated in hospitalized children and at a single time-point. We investigated the relationship between VLs and disease severity in both outpatients and inpatients with RSV infection.
We enrolled previously healthy children with RSV infection. Disease severity was defined by level of care (outpatients vs ward vs pediatric intensive care unit [PICU]), and a clinical disease severity score (CDSS). Nasopharyngeal VLs by polymerase chain reaction and CDSS were measured at enrollment and daily in inpatients. VL decay according to disease severity was analyzed using linear mixed modeling.
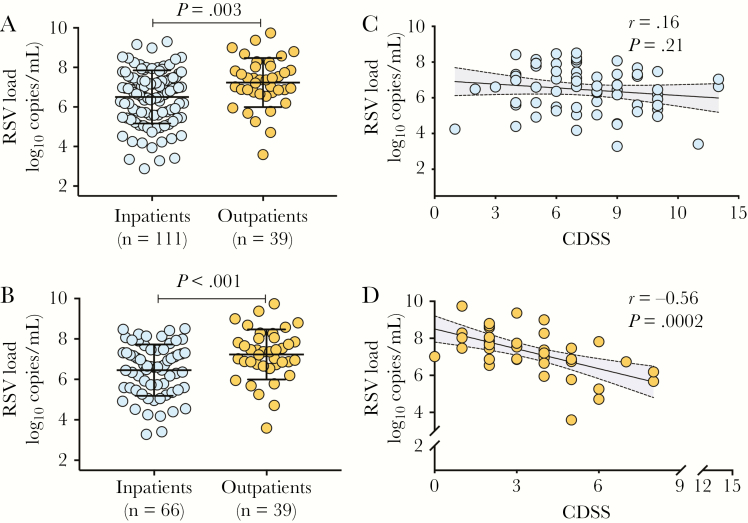
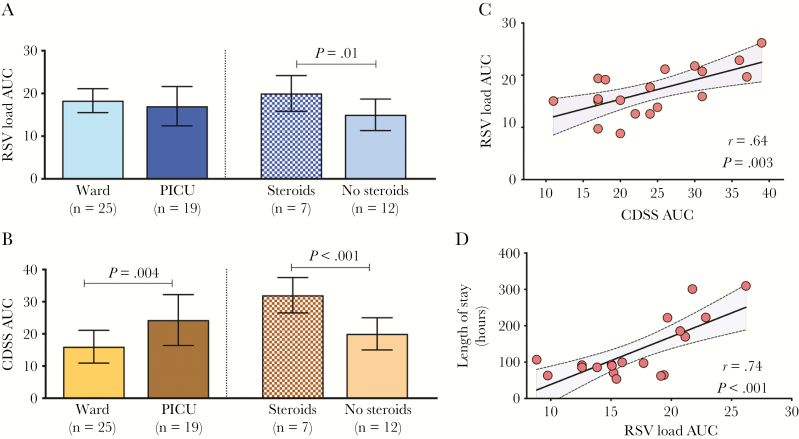
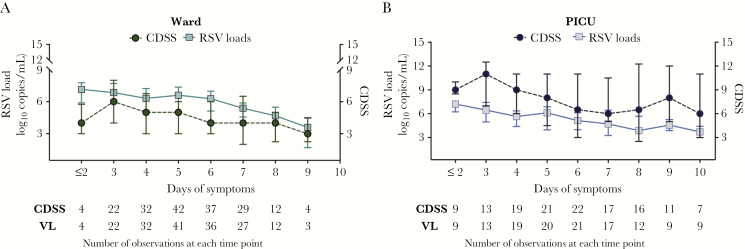
From February 2015 to March 2017, we enrolled 150 infants: 39 outpatients and 111 inpatients. VLs were higher in outpatients than in age-matched inpatients. Among inpatients, initial VLs were comparable in ward and PICU patients, and preceded the peak CDSS. However, after excluding infants treated with steroids, those hospitalized in the ward had higher VLs than infants requiring PICU care (P < .001). Dynamic analyses showed that VL decay was delayed in PICU patients, especially in those treated with steroids.
Higher VLs at presentation and a faster and consistent VL decline were both associated with less severe RSV disease in children.
Infants with less severe respiratory syncytial virus (RSV) disease had higher viral loads (VL) at presentation, and faster and consistent VL decline. Conversely, VL decay and overall viral exposure were prolonged and higher in infants severe RSV disease receiving steroids.
呼吸道合胞病毒(RSV)载量与儿童临床结局之间的关系仍有待确定。在大多数研究中,病毒载量(VL)是在住院患儿和单一时间点进行评估的。我们研究了门诊和住院 RSV 感染患儿的 VL 与疾病严重程度之间的关系。
我们招募了先前健康的 RSV 感染患儿。疾病严重程度通过护理级别(门诊 vs 病房 vs 儿科重症监护病房[PICU])和临床疾病严重程度评分(CDSS)来定义。入院时和住院期间每天通过聚合酶链反应检测鼻咽部 VL 和 CDSS。采用线性混合模型分析 VL 随疾病严重程度的衰减情况。
2015 年 2 月至 2017 年 3 月,我们共招募了 150 例婴儿:39 例门诊患儿和 111 例住院患儿。门诊患儿的 VL 高于年龄匹配的住院患儿。在住院患儿中,病房和 PICU 患儿的初始 VL 相当,且先于 CDSS 峰值。然而,在排除接受皮质类固醇治疗的患儿后,住院于病房的患儿的 VL 高于需要 PICU 治疗的患儿(P<.001)。动态分析显示,PICU 患儿的 VL 衰减延迟,尤其是接受皮质类固醇治疗的患儿。
在儿童中,较高的 VL 水平和更快、更一致的 VL 下降均与 RSV 疾病严重程度较轻有关。
RSV 疾病较轻的婴儿在就诊时具有更高的病毒载量(VL),且 VL 下降更快且更一致。相反,在接受皮质类固醇治疗的严重 RSV 疾病患儿中,VL 衰减和整体病毒暴露均延长且更高。