Service d'Hématologie Clinique et Thérapie Cellulaire, Univ.Bordeaux, INSERM U035, F-33000, Bordeaux, France.
Hematology Department (Torre F, planta 7), Hospital Universitario La Fe, Avinguda Fernando Abril Martorell, 106 CP, 46026, Valencia, Spain.
BMC Cancer. 2018 Nov 12;18(1):1100. doi: 10.1186/s12885-018-5002-5.
In acute lymphoblastic leukemia (ALL), the presence of minimal residual disease (MRD) after induction/consolidation chemotherapy is a strong prognostic factor for subsequent relapse and mortality. Accordingly, European clinical guidelines and protocols recommend testing patients who achieve a complete hematological remission (CR) for MRD for the purpose of risk stratification. The aim of this study was to provide quantitative information regarding real-world clinical practice for MRD testing in five European countries.
A web-based survey was conducted in March/April 2017 in France, Germany, Italy, Spain, and the UK. The survey was developed after consultation with specialist clinicians and a review of published literature. Eligible clinicians (20 per country; 23 in Spain) were board-certified in hemato-oncology or hematology, had at least five years' experience in their current role after training, had treated at least two patients with B-cell precursor ALL in the 12 months before the survey or at least five patients in the last five years, and had experience of testing for MRD in clinical practice.
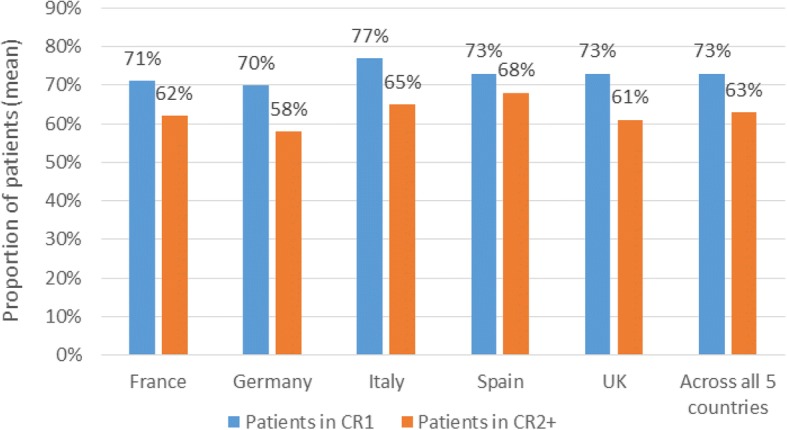
MRD testing is now standard practice in the treatment of adult ALL across the five European countries, with common use of recent treatment protocols which specify testing. Respondents estimated that, among clinicians in their country who conduct MRD testing, 73% of patients in first CR (CR1) and 63% of patients in second or later CR (CR2+) are tested for MRD. The median time point reported as most commonly used for the first MRD test, to establish risk status and to determine a treatment plan was four weeks after the start of induction therapy. The timing and frequency of tests is similar across countries. An average of four or five post-CR1 tests per patient in the 12 months after the first MRD test were reported across countries.
This comprehensive study of MRD testing patterns shows consistent practice across France, Germany, Italy, Spain, and the UK with respect to the timing and frequency of MRD testing, aligning with use of national protocols. MRD testing is used in clinical practice also in patients who reach CR2 + .
在急性淋巴细胞白血病(ALL)中,诱导/巩固化疗后微小残留病(MRD)的存在是后续复发和死亡的强烈预后因素。因此,欧洲临床指南和方案建议对达到完全血液学缓解(CR)的患者进行 MRD 检测,以进行风险分层。本研究的目的是为五个欧洲国家的 MRD 检测提供实际临床实践的定量信息。
2017 年 3 月/4 月在法国、德国、意大利、西班牙和英国进行了一项基于网络的调查。该调查是在与专家临床医生协商并审查已发表文献后制定的。合格的临床医生(每个国家 20 名;西班牙 23 名)在血液肿瘤学或血液学方面拥有董事会认证,在培训后的当前角色中至少有五年经验,在调查前 12 个月或过去五年中至少治疗过两名 B 细胞前体 ALL 患者,并且在临床实践中有 MRD 检测经验。
MRD 检测现在是五个欧洲国家治疗成人 ALL 的标准实践,普遍使用最近的治疗方案,这些方案规定了检测。受访者估计,在进行 MRD 检测的本国临床医生中,73%的首次 CR1(CR1)患者和 63%的第二次或更高 CR(CR2+)患者接受了 MRD 检测。报告的最常用于首次 MRD 检测以确定风险状况和制定治疗计划的中位时间点是诱导治疗开始后四周。各国的测试时间和频率相似。报告称,在首次 MRD 检测后的 12 个月内,每位患者平均进行四到五次 CR1 后检测。
这项关于 MRD 检测模式的综合研究表明,法国、德国、意大利、西班牙和英国在 MRD 检测的时间和频率方面存在一致的做法,与国家方案的使用一致。在达到 CR2+的患者中,MRD 检测也用于临床实践。