Lumlertgul Nuttha, Siribamrungwong Monchai, Jaber Bertrand L, Susantitaphong Paweena
Division of Nephrology, Department of Medicine, Faculty of Medicine, King Chulalongkorn Memorial Hospital, Chulalongkorn University, Bangkok, Thailand.
Department of Medicine, Lerdsin Hospital, College of Medicine, Rangsit University, Bangkok, Thailand.
Kidney Int Rep. 2018 Jul 29;3(6):1363-1372. doi: 10.1016/j.ekir.2018.07.020. eCollection 2018 Nov.
Little is known of the clinical outcomes of secondary oxalate nephropathy. To inform clinical practice, we performed a systematic review of case reports and case series to examine the clinical characteristics and outcomes of patients with secondary oxalate nephropathy.
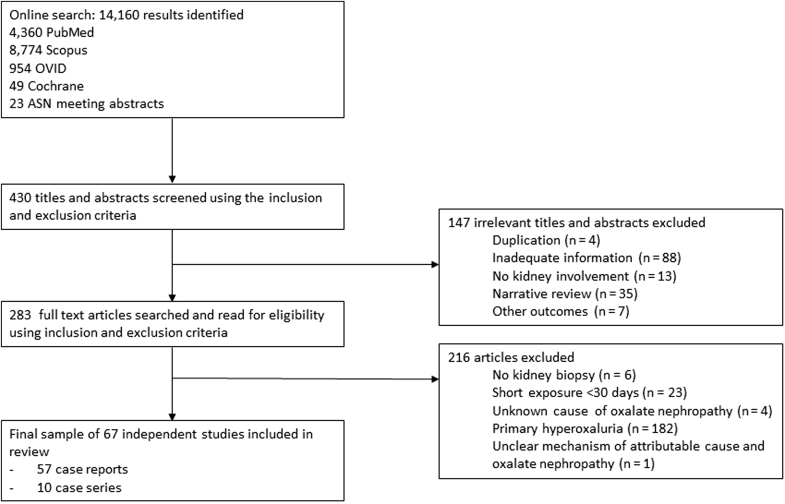
Electronic databases were searched for case reports and case series of individual cases or cohorts of patients with biopsy-proven oxalate nephropathy in native or transplanted kidneys from 1950 until January 2018.
Fifty-seven case reports and 10 case series met the inclusion criteria, totaling 108 patients. The case series were meta-analyzed. Mean age was 56.4 years old, 59% were men, and 15% were kidney transplant recipients. Fat malabsorption (88%) was the most commonly attributed cause of oxalate nephropathy, followed by excessive dietary oxalate consumption (20%). The mean baseline serum creatinine was 1.3 mg/dl and peaked at 4.6 mg/dl. Proteinuria, hematuria, and urinary crystals was reported in 69%, 32%, and 26% of patients, respectively. Mean 24-hour urinary oxalate excretion was 85.4 mg/d. In addition to universal oxalate crystal deposition in tubules and/or interstitium, kidney biopsy findings included acute tubular injury (71%), tubular damage and atrophy (69%), and interstitial mononuclear cell infiltration (72%); 55% of patients required dialysis. None had complete recovery, 42% had partial recovery, and 58% remained dialysis-dependent. Thirty-three percent of patients died.
Secondary oxalate nephropathy is a rare but potentially devastating condition. Renal replacement therapy is required in >50% of patients, and most patients remain dialysis-dependent. Studies are needed for effective preventive and treatment strategies in high-risk patients with hyperoxaluria-enabling conditions.
关于继发性草酸肾病的临床结局,人们了解甚少。为指导临床实践,我们对病例报告和病例系列进行了系统综述,以研究继发性草酸肾病患者的临床特征和结局。
检索电子数据库,查找1950年至2018年1月间经活检证实为天然肾或移植肾草酸肾病的个体病例或患者队列的病例报告和病例系列。
57篇病例报告和10个病例系列符合纳入标准,共计108例患者。对病例系列进行了荟萃分析。平均年龄为56.4岁,59%为男性,15%为肾移植受者。脂肪吸收不良(88%)是草酸肾病最常见的归因原因,其次是饮食中草酸摄入过多(20%)。平均基线血清肌酐为1.3mg/dl,峰值为4.6mg/dl。分别有69%、32%和26%的患者报告有蛋白尿、血尿和尿结晶。平均24小时尿草酸排泄量为85.4mg/d。除肾小管和/或间质普遍存在草酸晶体沉积外,肾活检结果还包括急性肾小管损伤(71%)、肾小管损伤和萎缩(69%)以及间质单核细胞浸润(72%);55%的患者需要透析。无一例完全康复,42%部分康复,58%仍依赖透析。33%的患者死亡。
继发性草酸肾病是一种罕见但可能具有毁灭性的疾病。超过50%的患者需要肾脏替代治疗,大多数患者仍依赖透析。需要开展研究以制定针对高草酸尿症相关疾病高危患者的有效预防和治疗策略。