Department of Surgical, Medical, Molecular and Critical Area Pathology, University of Pisa, Pisa, Italy.
Periodontology Unit, University College London Eastman Dental Institute, London, UK.
Int J Obes (Lond). 2019 May;43(5):1125-1129. doi: 10.1038/s41366-018-0253-4. Epub 2018 Nov 19.
To evaluate the effect of periodontitis (PD) on glucoregulatory hormones in obesity, never explored so far, a cross-sectional study was conducted in 110 severely obese, non-diabetic individuals.
We collected clinical periodontal parameters, including probing pocket depth (PPD), bleeding on probing (BOP), clinical attachment level (CAL). Insulin, glucagon, GLP-1 and GIP were measured after 3 days of standardized diet.
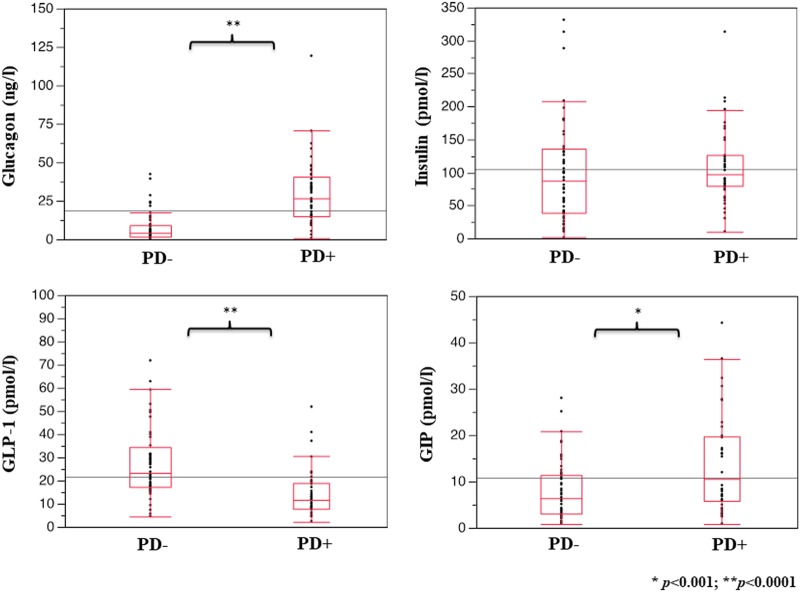
Forty-seven subjects had periodontitis (PD+) and 63 did not (PD-). PD+ showed 30.3% of gingival sites with PPD > 4 mm, 55.2% of BOP sites and a mean CAL loss of 4.1 mm. Compared with PD-, PD+ had higher glucagon (26.60 [25.22] vs 3.93 [7.50] ng/l, p < 0.0001) and GIP levels (10.56 [13.30] vs 6.43 [8.43] pmol/l, p < 0.001), while GLP-1 was reduced (11.78 [10.07] vs 23.34 [16.80] pmol/l, p < 0.0001). Insulin did not differ. In PD+, after adjustment for confounders, PPD was positively related to glucagon (β = 0.424, p = 0.002) and inversely to GLP-1 (β = -0.159, p = 0.044).
We describe for the first time an impaired incretin axis coupled with a relative hyperglucagonemia in obese non-diabetic individuals with PD, that might contribute to deteriorate their glucose tolerance and partially explain the higher risk of diabetes observed in these patients.
评估牙周炎(PD)对肥胖中尚未探索过的糖调节激素的影响,这是一项横断面研究,共纳入 110 名严重肥胖且非糖尿病的个体。
我们收集了临床牙周参数,包括探诊深度(PPD)、探诊出血(BOP)、临床附着水平(CAL)。在标准化饮食 3 天后测量胰岛素、胰高血糖素、GLP-1 和 GIP。
47 名受试者患有牙周炎(PD+),63 名受试者未患有牙周炎(PD-)。PD+有 30.3%的牙龈部位 PPD>4mm,55.2%的探诊出血部位,平均 CAL 丧失 4.1mm。与 PD-相比,PD+的胰高血糖素(26.60[25.22] vs 3.93[7.50]ng/l,p<0.0001)和 GIP 水平(10.56[13.30] vs 6.43[8.43]pmol/l,p<0.001)更高,而 GLP-1 降低(11.78[10.07] vs 23.34[16.80]pmol/l,p<0.0001)。胰岛素没有差异。在 PD+中,调整混杂因素后,PPD 与胰高血糖素呈正相关(β=0.424,p=0.002),与 GLP-1 呈负相关(β=-0.159,p=0.044)。
我们首次描述了肥胖非糖尿病个体中存在受损的肠促胰岛素轴,伴有相对高胰高血糖素血症,这可能导致其葡萄糖耐量恶化,并部分解释了这些患者糖尿病风险较高的原因。