Division of Nephrology and Clinical Immunology, RWTH Aachen University, Pauwelsstr. 30, 52074, Aachen, Germany.
Department of Intensive Care, RWTH Aachen University, Aachen, Germany.
BMC Nephrol. 2018 Nov 19;19(1):328. doi: 10.1186/s12882-018-1128-6.
The Oxford classification of IgA nephropathy (IgAN) defines histologic criteria (MEST-C) that provide prognostic information based on the kidney biopsy. There are few data on the predictive impact of this classification in randomized clinical trial settings.
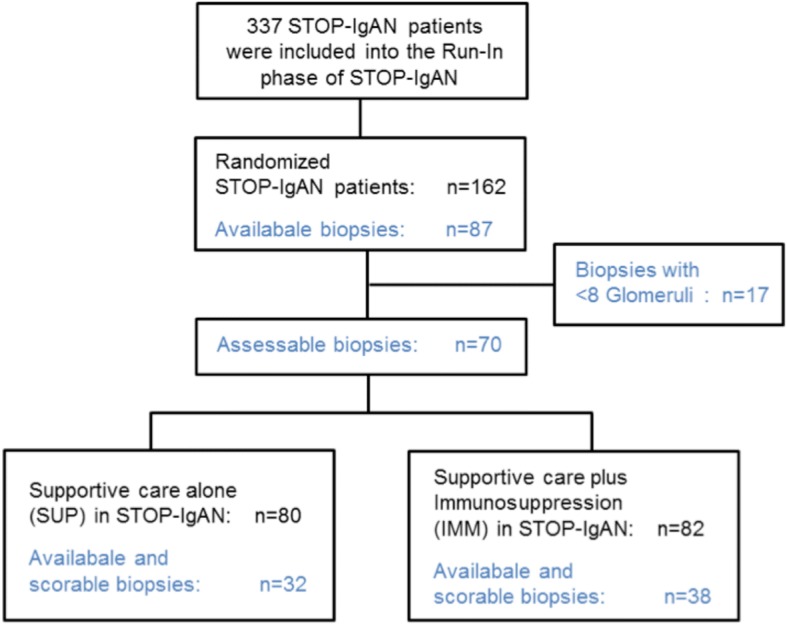
We performed an exploratory analysis of MEST-C scores in 70 available renal biopsies from 162 randomized STOP-IgAN trial participants and correlated the results with clinical outcomes. Analyses were performed by researchers blinded to the clinical outcome of the patients. Biopsies had been obtained 6.5 to 95 (median 9.4) months prior to randomization.
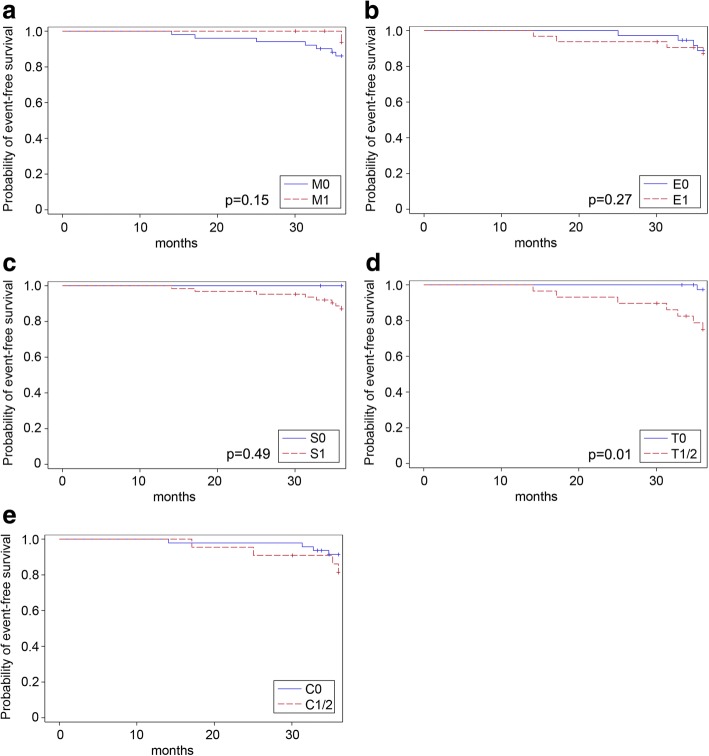
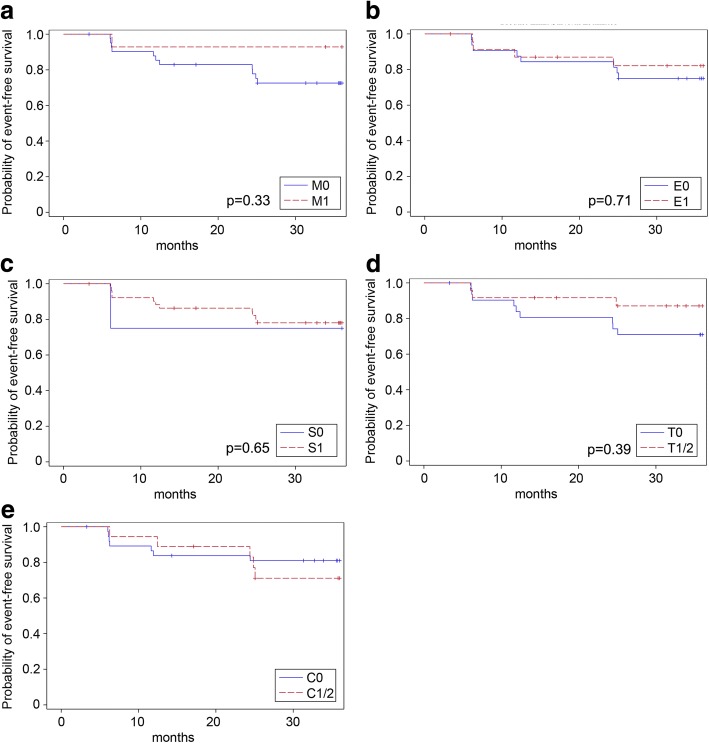
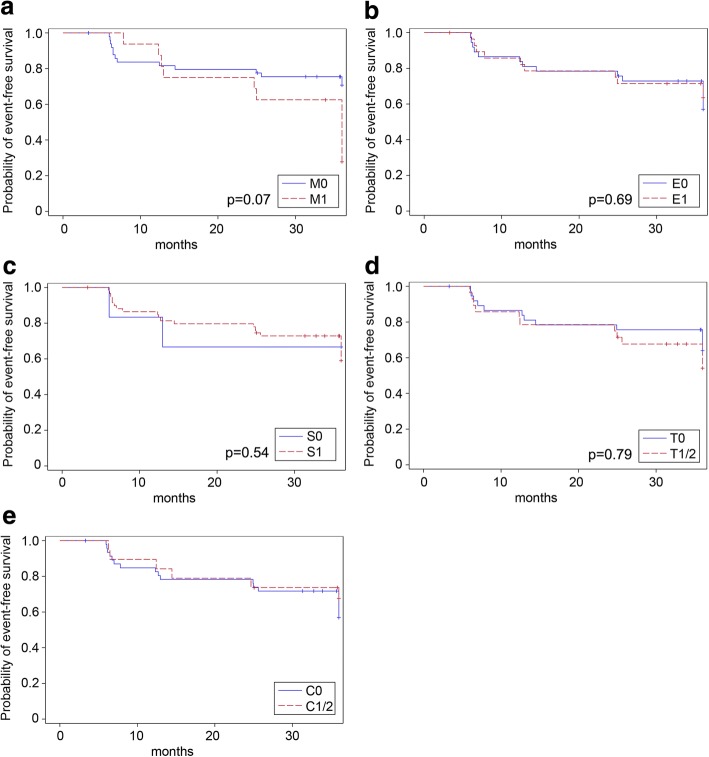
Mesangial hypercellularity (M1) associated with higher annual eGFR-loss during the 3-year trial (M1: - 5.06 ± 5.17 ml/min/1.73 m, M0: - 0.79 ± 4.50 ml/min/1.73 m, p = 0.002). An M0-score additionally showed a weak association with full clinical remission, whereas the percentage of patients losing ≥15 ml/min/1.73 m over the 3-year trial phase was higher among those scored as M1. Among patients with additional immunosuppression, ESRD occurred more frequently in patients when tubulointerstitial fibrosis (T1/2) was present (T1/2 = 33%, T0 = 0%, p = 0.008). In patients receiving supportive care only, ESRD frequencies were similar (T1/2 = 18%, T0 = 7%, p = 0.603). At randomization, eGFR was significantly lower when tubulointerstitial fibrosis was present (T1/2: 45.2 ± 15.7 ml/min/1.73 m, T0: 74.6 ± 28.2 ml/min/1.73 m, p < 0.0001). Endocapillary hypercellularity (E), and glomerular segmental sclerosis (S) were not associated with any clinical outcome parameter. In the analyzed cohort, patients with glomerular crescents (C1/2 scores) in their biopsies were more likely to develop ESRD during the 3-year trial phase, but this trend was only significant in patients under supportive care.
This secondary analysis of STOP-IgAN biopsies indicates that M1, T1/2 and C1/2 scores associate with worse renal outcomes.
牛津 IgA 肾病分类(IgAN)定义了组织学标准(MEST-C),这些标准基于肾活检提供预后信息。关于该分类在随机临床试验中的预测影响的数据很少。
我们对 162 名 STOP-IgAN 试验参与者的 70 份可获得的肾活检进行了 MEST-C 评分的探索性分析,并将结果与临床结果相关联。分析是由对患者临床结果不知情的研究人员进行的。活检是在随机分组前 6.5 至 95 个月(中位数 9.4 个月)进行的。
系膜细胞增生(M1)与 3 年试验期间的年 eGFR 损失更高相关(M1:-5.06±5.17 ml/min/1.73 m,M0:-0.79±4.50 ml/min/1.73 m,p=0.002)。M0 评分还与完全临床缓解弱相关,而在 3 年试验阶段中,那些评分 M1 的患者中,有更多的患者失去了≥15 ml/min/1.73 m。在接受额外免疫抑制的患者中,当存在肾小管间质纤维化(T1/2)时,ESRD 更常见(T1/2=33%,T0=0%,p=0.008)。在仅接受支持性治疗的患者中,ESRD 的频率相似(T1/2=18%,T0=7%,p=0.603)。随机分组时,存在肾小管间质纤维化时 eGFR 显著降低(T1/2:45.2±15.7 ml/min/1.73 m,T0:74.6±28.2 ml/min/1.73 m,p<0.0001)。内皮下细胞增生(E)和肾小球节段性硬化(S)与任何临床结局参数均无关联。在分析的队列中,活检中有肾小球新月体(C1/2 评分)的患者在 3 年试验期间更有可能发展为 ESRD,但这种趋势仅在接受支持性治疗的患者中显著。
这项 STOP-IgAN 活检的二次分析表明,M1、T1/2 和 C1/2 评分与更差的肾脏结局相关。