Department of Pediatrics, Jinling Hospital, The First School of Clinical Medicine, Southern Medical University, Nanjing, China.
Department of Pediatrics, Nanfang Hospital, Southern Medical University, Guangzhou, China.
BMC Nephrol. 2020 Jul 1;21(1):247. doi: 10.1186/s12882-020-01913-7.
The 2016 Oxford Classification's MEST-C scoring system predicts outcomes in adults with IgA nephropathy (IgAN), but it lacks tremendous cohort validation in children with IgAN in China. We sought to verify whether the Oxford classification could be used to predict the renal outcome of children with IgAN.
In this retrospective cohort study, 1243 Chinese IgAN children who underwent renal biopsy in Jinling Hospital were enregistered from 2000 to 2017. The combined endpoint was defined as either a ≥ 50% reduction in estimated glomerular filtration rate (eGFR) or end-stage renal disease (ESRD). We probed into the relevance betwixt the Oxford classification and renal prognosis.
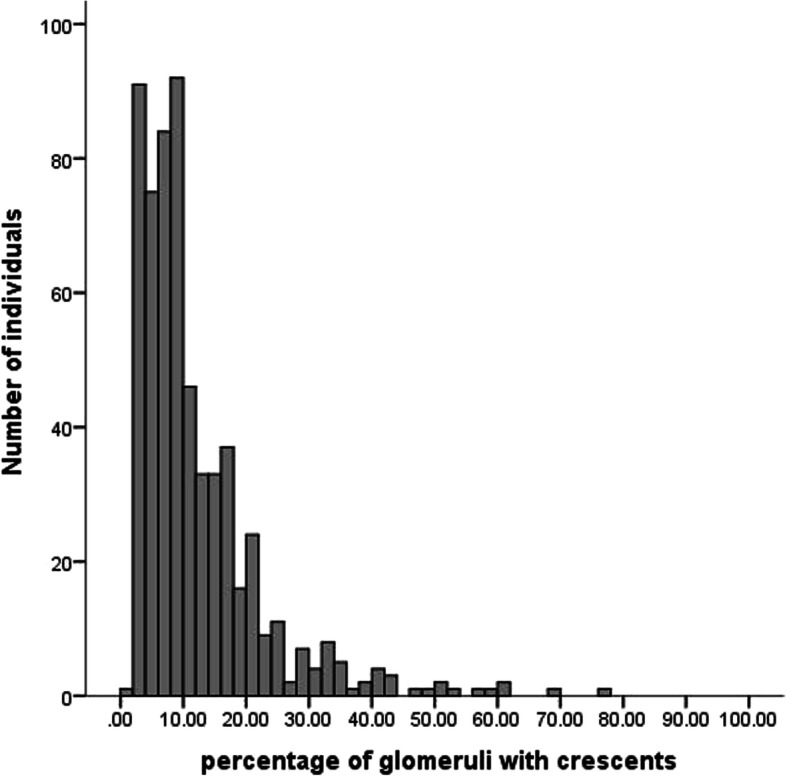
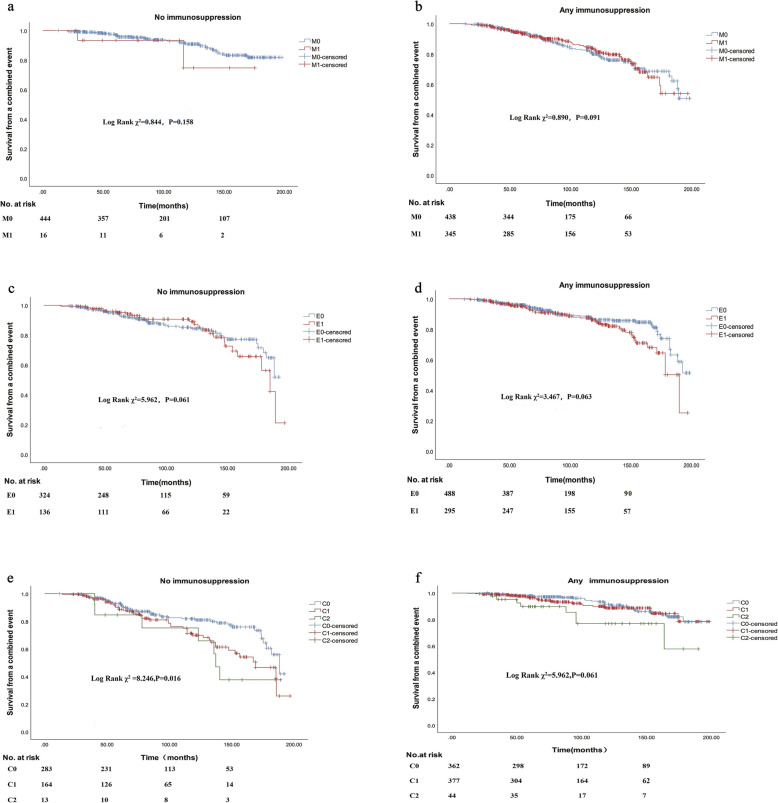
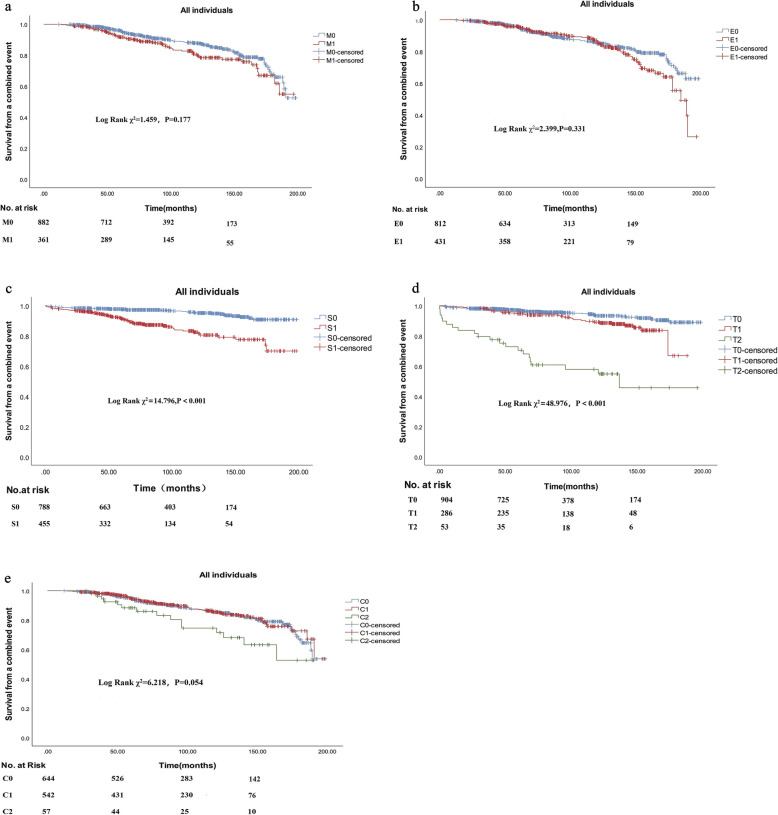
There were 29% of children with mesangial proliferation(M1), 35% with endocapillary proliferation (E1), 37% with segmental sclerosis/adhesion lesion (S1), 23% with moderate tubular atrophy/interstitial fibrosis (T1 25-50% of cortical area involved), 4.3% with severe tubular atrophy/interstitial fibrosis (T2 > 50% of cortical area involved), 44% with crescent in< 25% of glomeruli(C1), and 4.6% with crescent in> 25% of glomeruli (C2). All children were followed for a medial of 7.2 (4.6-11.7) years, 171 children (14%) arrived at the combined endpoint. The multivariate COX regression model revealed that the presence of lesions S (HR2.7,95%CI 1.8 ~ 4.2, P<0.001) and T (HR6.6,95%CI 3.9 ~ 11.3, P<0.001) may be the reason for poorer prognosis in the whole cohort. In contrast, C lesion showed a significant association with the outcome only in children received no immunosuppressive treatment.
This study revealed that S and T lesions were useful as the long-term renal prognostic factors among Chinese IgAN children.
2016 年牛津分类的 MEST-C 评分系统预测了成人 IgA 肾病(IgAN)的结局,但它在中国 IgAN 患儿中缺乏大量的队列验证。我们试图验证牛津分类是否可用于预测 IgAN 患儿的肾脏结局。
在这项回顾性队列研究中,我们登记了 2000 年至 2017 年在南京军区南京总医院行肾活检的 1243 例中国 IgAN 患儿。联合终点定义为估算肾小球滤过率(eGFR)下降≥50%或终末期肾病(ESRD)。我们探讨了牛津分类与肾脏预后之间的相关性。
系膜增殖(M1)患儿占 29%,内皮下增殖(E1)占 35%,节段性硬化/黏附病变(S1)占 37%,中-重度肾小管萎缩/间质纤维化(T1 累及 25%-50%皮质区)占 23%,严重肾小管萎缩/间质纤维化(T2 累及>50%皮质区)占 4.3%,新月体病变<25%肾小球(C1)占 44%,新月体病变>25%肾小球(C2)占 4.6%。所有患儿的中位随访时间为 7.2(4.6-11.7)年,171 例患儿(14%)达到联合终点。多变量 COX 回归模型显示,病变 S(HR2.7,95%CI 1.84.2,P<0.001)和 T(HR6.6,95%CI 3.911.3,P<0.001)的存在可能是全队列预后不良的原因。相比之下,仅在未接受免疫抑制治疗的患儿中,C 病变与结局有显著相关性。
本研究表明,S 和 T 病变是中国 IgAN 患儿长期肾脏预后的有用因素。