Zakaria Wael K, Hafez Raef F, Taha Ahmed N
Department of Neurosurgery, Mansoura University Hospital, Mansoura, International Medical Center, Cairo, Egypt.
Asian J Neurosurg. 2018 Oct-Dec;13(4):1037-1041. doi: 10.4103/ajns.AJNS_61_17.
Skull base chordomas are locally invasive tumors which able to extend in different directions with skull base invasion. Although they are histologically benign, they have invasive nature makes total resection virtually impossible to achieve in most cases and this lead to residual tumors after surgery. To decrease postoperative surgical resection morbidity of these tumors, gamma knife radiosurgery (GKRS) was performed as alternative management for these residual chordomas to evaluate its safety and efficacy.
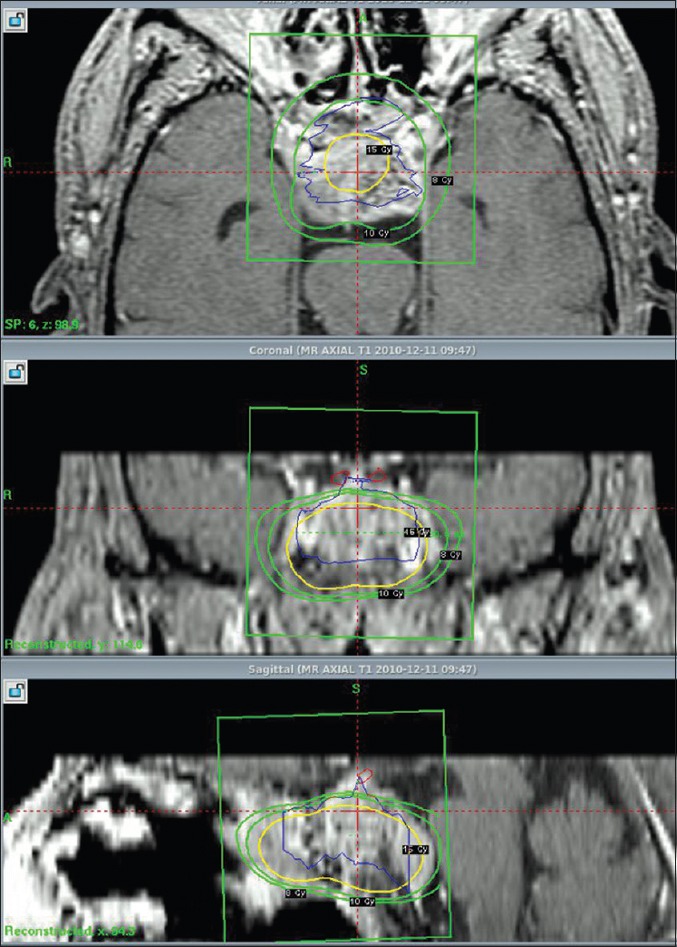
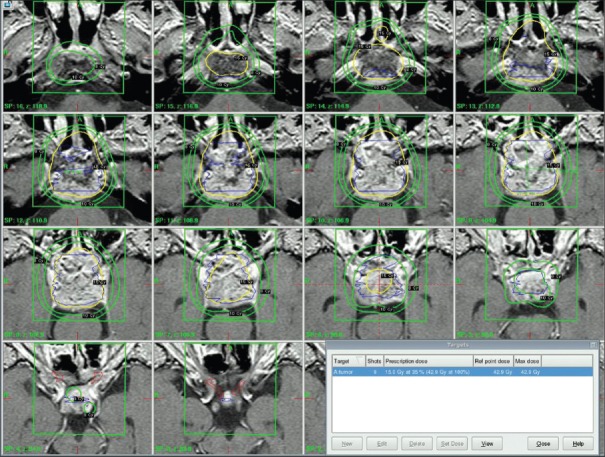
A retrospective study was made on eight residual skull base chordomas treated with GKRS between 2011 and 2015. The mean patient age was 49 years (range 30-73 years). Four patients harboring chordoma were male, and four patients were females with 1:1 ratio. All patients had undergone one prior surgery. Patients were treated with peripheral dose ranged between 12-15 gray (Gy) (mean 13.75 Gy) usually at 35% to 50% isodose curve (mean 38.8%). The maximum dose to the adjacent brain stem area ranged between 10 and 12 Gy. All patients were followed up from 8 to 39 months (mean 18 months).
The tumor control rate was 50% and 25% after 18 and 36 months, respectively, but we found that their wasdeclined in the tumor control rate with long follow-up time. Four tumors were stable in their size just for 18 months, and then there two of these tumors were progressed in their size, the other four patients showed progression in their tumors in their 1 year of treatment without sign of central tumor necrosis.
Skull base chordoma patients complained from symptoms due to tumor mass effect which were not prospected to respond to GKRS alone as the aim of this type of treatment was the local tumor control, the tumor control rate declined with long follow-up time and this correlated with radioresistant nature of skull base chordoma. We advise a gross total resection to decrease the tumor volume, and this making gamma knife a reasonable treatment modality.
颅底脊索瘤是具有局部侵袭性的肿瘤,能够向不同方向扩展并侵犯颅底。尽管它们在组织学上是良性的,但因其具有侵袭性,在大多数情况下几乎不可能实现完全切除,这导致术后残留肿瘤。为降低这些肿瘤术后手术切除的发病率,采用伽玛刀放射外科治疗(GKRS)作为这些残留脊索瘤的替代治疗方法,以评估其安全性和有效性。
对2011年至2015年间接受GKRS治疗的8例残留颅底脊索瘤进行回顾性研究。患者平均年龄为49岁(范围30 - 73岁)。患有脊索瘤的患者中4例为男性,4例为女性,比例为1:1。所有患者均曾接受过一次手术。患者接受的外周剂量范围为12 - 15格雷(Gy)(平均13.75 Gy),通常在35%至50%等剂量曲线(平均38.8%)。相邻脑干区域的最大剂量范围为10至12 Gy。所有患者随访8至39个月(平均18个月)。
18个月和36个月后的肿瘤控制率分别为50%和25%,但我们发现随着随访时间延长,肿瘤控制率有所下降。4个肿瘤大小仅在18个月内保持稳定,之后其中2个肿瘤大小进展,另外4例患者在治疗1年内肿瘤进展,且无中央肿瘤坏死迹象。
颅底脊索瘤患者因肿瘤占位效应出现症状,由于这种治疗的目的是局部肿瘤控制,预计单独的GKRS对这些症状无效,随着随访时间延长肿瘤控制率下降,这与颅底脊索瘤的放射抵抗性相关。我们建议进行全切除以减小肿瘤体积,这使得伽玛刀成为一种合理的治疗方式。