Academic Unit of Surgery, University of Glasgow, Glasgow, United Kingdom.
J Cachexia Sarcopenia Muscle. 2019 Feb;10(1):111-122. doi: 10.1002/jcsm.12357. Epub 2018 Nov 20.
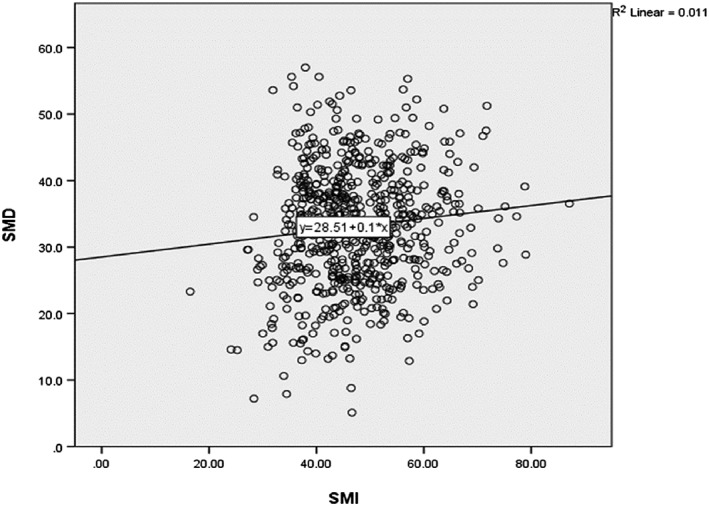
Colorectal cancer is the fourth leading cause of cancer mortality in developed countries. There is evidence supporting a disproportionate loss of skeletal muscle as an independent prognostic factor. The importance of the systemic inflammatory response as a unifying mechanism for specific loss of skeletal muscle mass in patients with cancer is increasingly recognized. The aim of the present study was to delineate the relationship between the systemic inflammatory response, skeletal muscle index (SMI), skeletal muscle density (SMD), and overall survival in patients with colorectal cancer.
The study included 650 patients with primary operable colorectal cancer. Computed tomography scans were used to define the presence of visceral obesity, sarcopenia (low SMI), and myosteatosis (low SMD). Tumour and patient characteristics were recorded. Survival analysis was carried out using univariate and multivariate Cox regression.
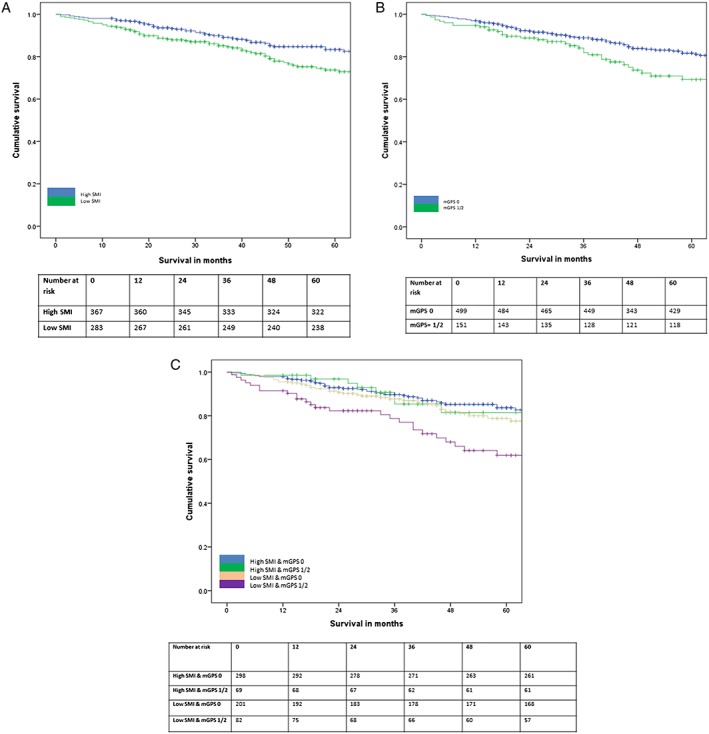
A total of 650 patients (354 men and 296 women) were included. The majority of patients were over 65 years of age (64%) and overweight or obese (68%). On univariate survival analysis, age, ASA, TNM stage, modified Glasgow Prognostic Score (mGPS), body mass index, subcutaneous fat index, visceral obesity, SMI, and SMD were significantly associated with overall survival (all P < 0.05). A low SMI and SMD were significantly associated with an elevated mGPS (<0.05). On multivariate analysis, SMI (Martin) [hazard ratio (HR) 1.50, 95% confidence interval (CI) 1.04-2.18, P = 0.031], SMD (Xiao) (HR 1.42, 95% CI 0.98-2.05, P = 0.061), and mGPS (HR 1.44, 95% CI 1.15-1.79, P = 0.001) were independently associated with overall survival. SMD but not SMI was significantly associated with ASA (P < 0.001).
This study delineates the relationship between the loss of quantity and quality of skeletal muscle mass, the systemic inflammatory response, and survival in patients with operable colorectal cancer.
结直肠癌是发达国家癌症死亡的第四大主要原因。有证据表明,骨骼肌的大量丢失是一个独立的预后因素。人们越来越认识到,全身炎症反应是癌症患者特定骨骼肌质量丢失的统一机制。本研究旨在描绘结直肠癌患者全身炎症反应、骨骼肌指数(SMI)、骨骼肌密度(SMD)与总生存之间的关系。
该研究纳入了 650 例原发性可手术结直肠癌患者。使用计算机断层扫描来确定内脏肥胖、肌肉减少症(低 SMI)和肌内脂肪增多(低 SMD)的存在。记录肿瘤和患者特征。使用单因素和多因素 Cox 回归进行生存分析。
共纳入 650 例患者(354 例男性和 296 例女性)。大多数患者年龄超过 65 岁(64%),超重或肥胖(68%)。单因素生存分析显示,年龄、ASA 分级、TNM 分期、改良格拉斯哥预后评分(mGPS)、体重指数、皮下脂肪指数、内脏肥胖、SMI 和 SMD 与总生存均显著相关(均 P<0.05)。低 SMI 和 SMD 与 mGPS 升高显著相关(P<0.05)。多因素分析显示,SMI(Martin)[风险比(HR)1.50,95%置信区间(CI)1.04-2.18,P=0.031]、SMD(Xiao)(HR 1.42,95%CI 0.98-2.05,P=0.061)和 mGPS(HR 1.44,95%CI 1.15-1.79,P=0.001)与总生存独立相关。SMD 与 ASA 显著相关(P<0.001),而 SMI 则不然。
本研究阐明了可手术结直肠癌患者骨骼肌质量数量和质量损失、全身炎症反应与生存之间的关系。