Department of Medicine, School of Medicine, Indiana University, Indianapolis, Indiana.
Department of Medicine, Center for Aging Research, Indiana University, Indianapolis, Indiana.
J Am Geriatr Soc. 2018 Dec;66(12):2289-2297. doi: 10.1111/jgs.15640. Epub 2018 Nov 21.
To assess the efficacy of haloperidol in reducing postoperative delirium in individuals undergoing thoracic surgery.
Randomized double-blind placebo-controlled trial.
Surgical intensive care unit (ICU) of tertiary care center.
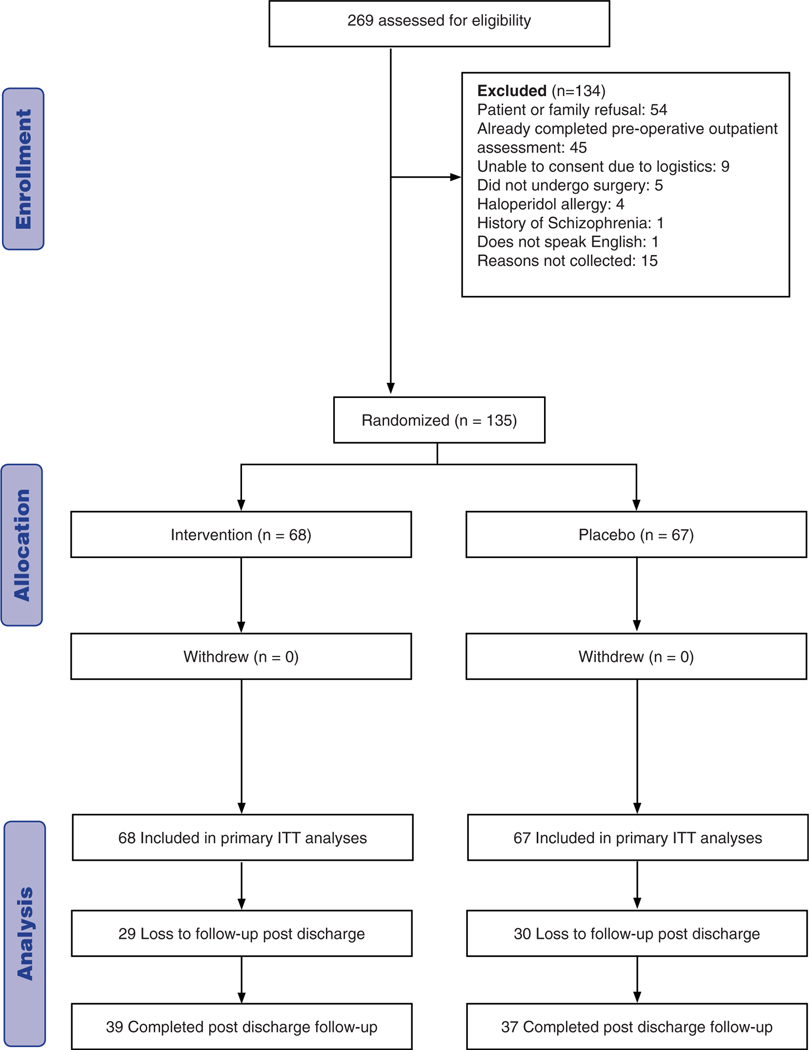
Individuals undergoing thoracic surgery (N=135).
Low-dose intravenous haloperidol (0.5 mg three times daily for a total of 11 doses) administered postoperatively.
The primary outcome was delirium incidence during hospitalization. Secondary outcomes were time to delirium, delirium duration, delirium severity, and ICU and hospital length of stay. Delirium was assessed using the Confusion Assessment Method for the ICU and delirium severity using the Delirium Rating Scale-Revised.
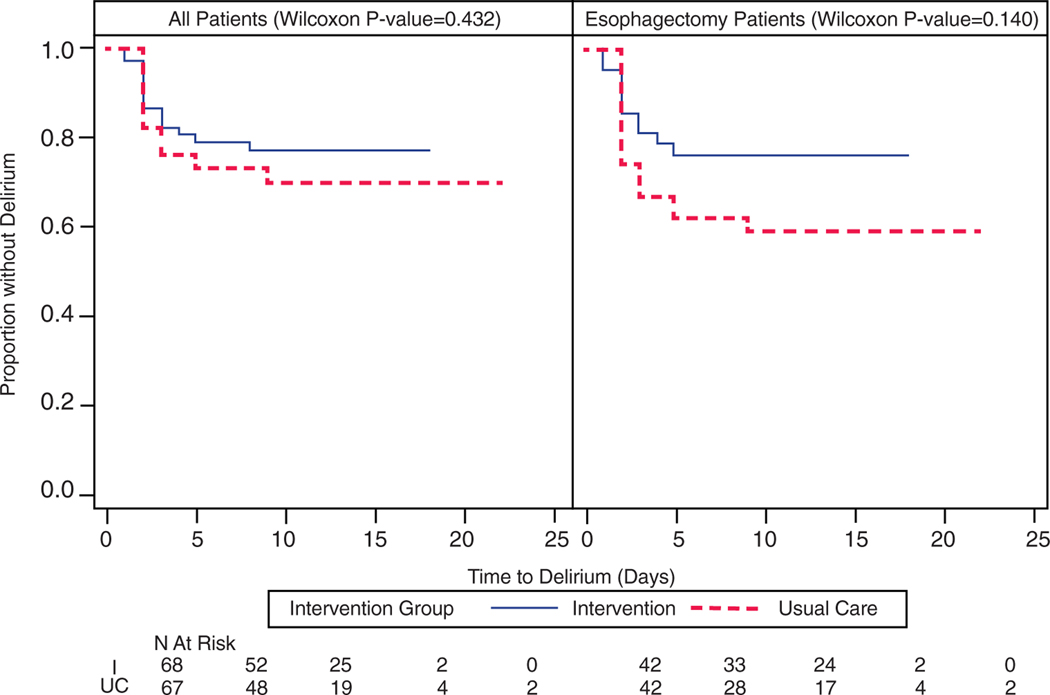
Sixty-eight participants were randomized to receive haloperidol and 67 placebo. No significant differences were observed between those receiving haloperidol and those receiving placebo in incident delirium (n=15 (22.1%) vs n=19 (28.4%); p = .43), time to delirium (p = .43), delirium duration (median 1 day, interquartile range (IQR) 1-2 days vs median 1 day, IQR 1-2 days; p = .71), delirium severity, ICU length of stay (median 2.2 days, IQR 1-3.3 days vs median 2.3 days, IQR 1-4 days; p = .29), or hospital length of stay (median 10 days, IQR 8-11.5 days vs median 10 days, IQR 8-12 days; p = .41). In the esophagectomy subgroup (n = 84), the haloperidol group was less likely to experience incident delirium (n=10 (23.8%) vs n=17 (40.5%); p = .16). There were no differences in time to delirium (p = .14), delirium duration (median 1 day, IQR 1-2 days vs median 1 day, IQR 1-2 days; p = .71), delirium severity, or hospital length of stay (median 11 days, IQR 10-12 days vs median days 11, IQR 10-15 days; p = .26). ICU length of stay was significantly shorter in the haloperidol group (median 2.8 days, IQR 1.1-3.8 days vs median 3.1 days, IQR 2.1-5.1 days; p = .03). Safety events were comparable between the groups.
Low-dose postoperative haloperidol did not reduce delirium in individuals undergoing thoracic surgery but may be efficacious in those undergoing esophagectomy. J Am Geriatr Soc 66:2289-2297, 2018.
评估小剂量氟哌啶醇在减少接受胸外科手术患者术后谵妄中的疗效。
随机、双盲、安慰剂对照试验。
三级护理中心的外科重症监护病房(ICU)。
接受胸外科手术的个体(N=135)。
术后给予低剂量静脉氟哌啶醇(0.5mg,每日 3 次,共 11 剂)。
主要结局为住院期间谵妄发生率。次要结局为谵妄发生时间、谵妄持续时间、谵妄严重程度以及 ICU 和住院时间。使用 ICU 意识混乱评估方法和修订后的谵妄严重程度评估量表评估谵妄。
68 名参与者被随机分配接受氟哌啶醇治疗,67 名接受安慰剂治疗。接受氟哌啶醇治疗的患者与接受安慰剂治疗的患者在谵妄发生率(n=15(22.1%)与 n=19(28.4%);p=0.43)、谵妄发生时间(p=0.43)、谵妄持续时间(中位数 1 天,四分位距(IQR)1-2 天与中位数 1 天,IQR 1-2 天;p=0.71)、谵妄严重程度、ICU 住院时间(中位数 2.2 天,IQR 1-3.3 天与中位数 2.3 天,IQR 1-4 天;p=0.29)或住院时间(中位数 10 天,IQR 8-11.5 天与中位数 10 天,IQR 8-12 天;p=0.41)方面无显著差异。在食管切除术亚组(n=84)中,氟哌啶醇组发生谵妄的可能性较低(n=10(23.8%)与 n=17(40.5%);p=0.16)。在谵妄发生时间(p=0.14)、谵妄持续时间(中位数 1 天,IQR 1-2 天与中位数 1 天,IQR 1-2 天;p=0.71)、谵妄严重程度或住院时间(中位数 11 天,IQR 10-12 天与中位数 11 天,IQR 10-15 天;p=0.26)方面无差异。氟哌啶醇组 ICU 住院时间显著缩短(中位数 2.8 天,IQR 1.1-3.8 天与中位数 3.1 天,IQR 2.1-5.1 天;p=0.03)。两组安全性事件相当。
术后小剂量氟哌啶醇并不能减少胸外科手术患者的谵妄,但可能对接受食管切除术的患者有效。美国老年医学会 66:2289-2297,2018。