Friedrich-Alexander University Erlangen-Nürnberg (FAU), Department of Neurology, Schwabachanlage 6, 91054, Erlangen, Germany.
Crit Care. 2018 Nov 21;22(1):317. doi: 10.1186/s13054-018-2235-2.
Patients in refractory status epilepticus (RSE) may require treatment with continuous intravenous anesthetic drugs (cIVADs) for seizure control. The use of cIVADs, however, was recently associated with poor outcome in status epilepticus (SE), raising the question of whether cIVAD therapy should be delayed for attempts to halt seizures with repeated non-anesthetic antiepileptic drugs. In this study, we aimed to determine the impact of differences in therapeutic approaches on RSE outcome using timing of cIVAD therapy as a surrogate for treatment aggressiveness.
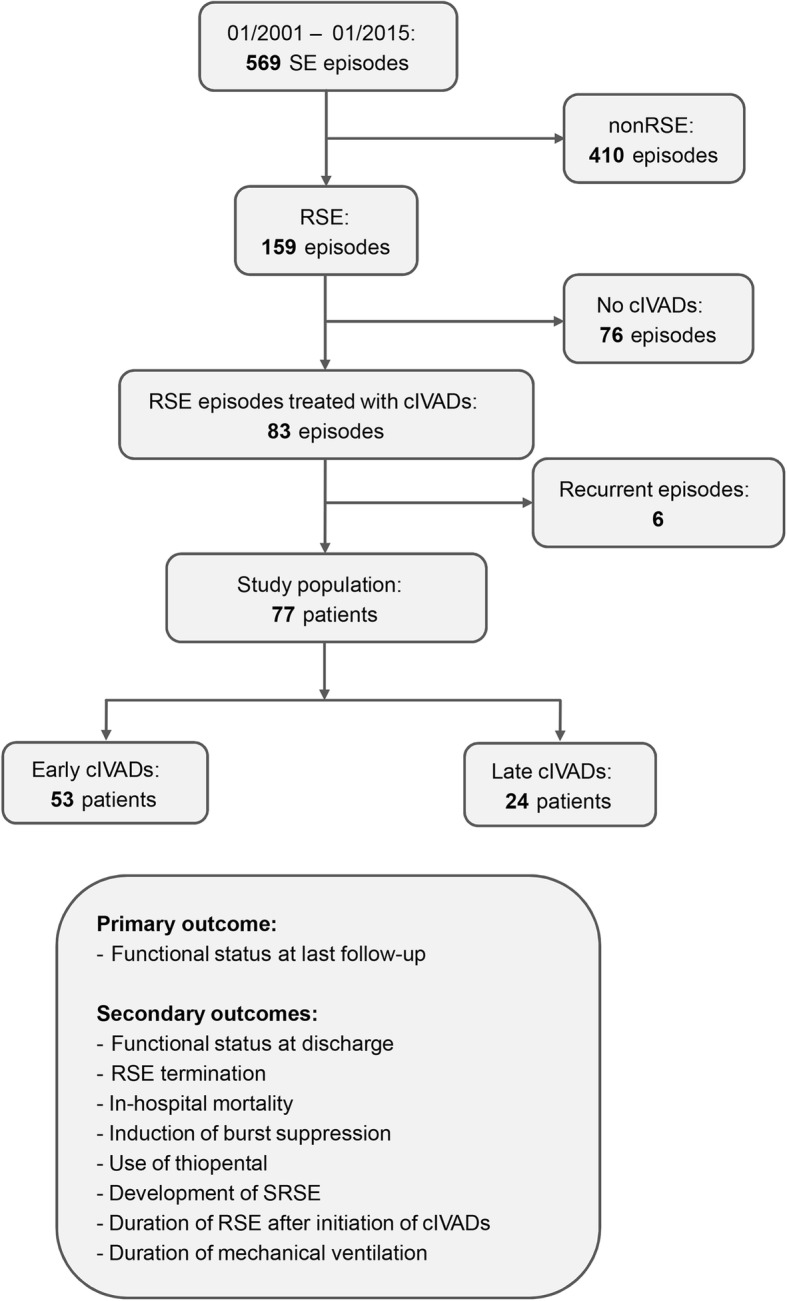
This was a retrospective cohort study over 14 years (n = 77) comparing patients with RSE treated with cIVADs within and after 48 h after RSE onset, and functional status at last follow-up was the primary outcome (good = return to premorbid baseline or modified Rankin Scale score of less than 3). Secondary outcomes included discharge functional status, in-hospital mortality, RSE termination, induction of burst suppression, use of thiopental, duration of RSE after initiation of cIVADs, duration of mechanical ventilation, and occurrence of super-refractory SE. Analysis was performed on the total cohort and on subgroups defined by RSE severity according to the Status Epilepticus Severity Score (STESS) and by the variables contained therein.
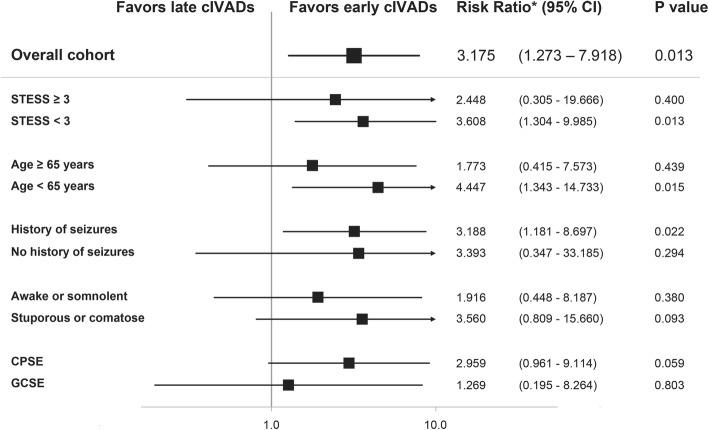
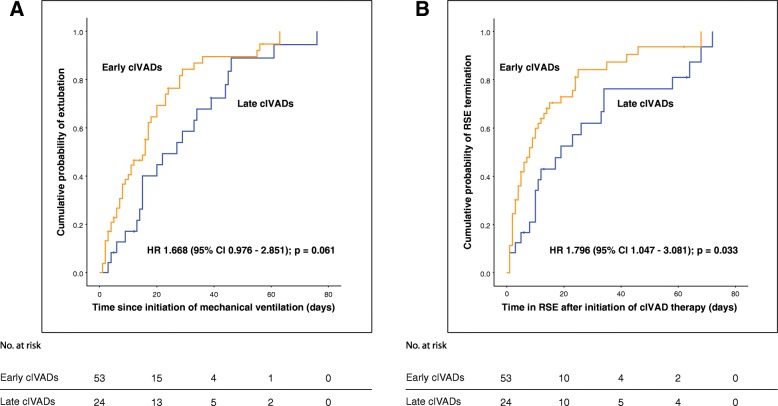
Fifty-three (68.8%) patients received cIVADs within the first 48 h. Early cIVAD treatment was independently associated with good outcome (adjusted risk ratio [aRR] 3.175, 95% confidence interval [CI] 1.273-7.918; P = 0.013) as well as lower chance of both induction of burst suppression (aRR 0.661, 95% CI 0.507-0.861; P = 0.002) and use of thiopental (aRR 0.446, 95% CI 0.205-0.874; P = 0.043). RSE duration after cIVAD initiation was shorter in the early cIVAD cohort (hazard ratio 1.796, 95% CI 1.047-3.081; P = 0.033). Timing of cIVAD use did not impact the remaining secondary outcomes. Subgroup analysis revealed early cIVAD impact on the primary outcome to be driven by patients with STESS of less than 3.
Patients with RSE treated with cIVADs may benefit from early initiation of such therapy.
难治性癫痫持续状态(RSE)患者可能需要持续静脉注射麻醉药物(cIVAD)来控制癫痫发作。然而,最近 cIVAD 的使用与癫痫持续状态(SE)的不良预后相关,这引发了一个问题,即是否应该延迟 cIVAD 治疗,以便尝试用重复的非麻醉性抗癫痫药物来停止癫痫发作。在这项研究中,我们旨在通过将 cIVAD 治疗的时间作为治疗强度的替代指标,来确定治疗方法的差异对 RSE 结局的影响。
这是一项回顾性队列研究,时间跨度为 14 年(n = 77),比较了在 RSE 发作后 48 小时内和之后接受 cIVAD 治疗的 RSE 患者,主要结局是最后一次随访时的功能状态(良好=恢复到发病前基线或改良 Rankin 量表评分小于 3)。次要结局包括出院时的功能状态、住院死亡率、RSE 终止、诱导爆发抑制、使用硫喷妥钠、cIVAD 开始后 RSE 的持续时间、机械通气时间和发生超难治性 SE 的情况。分析在总队列和根据癫痫持续状态严重程度评分(STESS)和其中包含的变量定义的亚组中进行。
53 名(68.8%)患者在最初的 48 小时内接受了 cIVAD 治疗。早期 cIVAD 治疗与良好的结局独立相关(调整风险比[aRR]3.175,95%置信区间[CI]1.273-7.918;P = 0.013),同时也降低了诱导爆发抑制(aRR 0.661,95%CI 0.507-0.861;P = 0.002)和使用硫喷妥钠(aRR 0.446,95%CI 0.205-0.874;P = 0.043)的可能性。在早期 cIVAD 组,cIVAD 开始后 RSE 的持续时间更短(风险比 1.796,95%CI 1.047-3.081;P = 0.033)。cIVAD 使用时间对其余次要结局没有影响。亚组分析显示,早期 cIVAD 对主要结局的影响是由 STESS 小于 3 的患者驱动的。
接受 cIVAD 治疗的 RSE 患者可能受益于早期开始这种治疗。