Department of Anesthesiology and Critical Care Medicine, Saint-Antoine Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France.
Sorbonne University, INSERM, Institut Pierre Louis d'Epidémiologie et de Santé Publique IPLESP, Public Health Department, Saint-Antoine Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France.
Crit Care. 2018 Nov 22;22(1):321. doi: 10.1186/s13054-018-2256-x.
Infected pancreatic necrosis, which occurs in about 40% of patients admitted for acute necrotizing pancreatitis, requires combined antibiotic therapy and local drainage. Since 2010, drainage by open surgical necrosectomy has been increasingly replaced by less invasive methods such as percutaneous radiological drainage, endoscopic necrosectomy, and laparoscopic surgery, which proved effective in small randomized controlled trials in highly selected patients. Few studies have evaluated minimally invasive drainage methods used under the conditions of everyday hospital practice. The aim of this study was to determine whether, compared with conventional open surgery, minimally invasive drainage was associated with improved outcomes of critically ill patients with infection complicating acute necrotizing pancreatitis.
A single-center observational study was conducted in patients admitted to the intensive care unit for severe acute necrotizing pancreatitis to compare the characteristics, drainage techniques, and outcomes of the 62 patients managed between September 2006 and December 2010, chiefly with conventional open surgery, and of the 81 patients managed between January 2011 and August 2015 after the introduction of a minimally invasive drainage protocol.
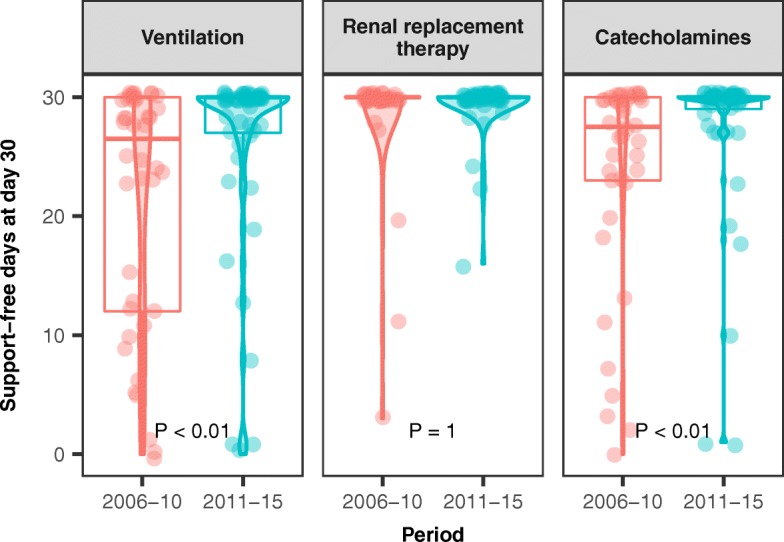
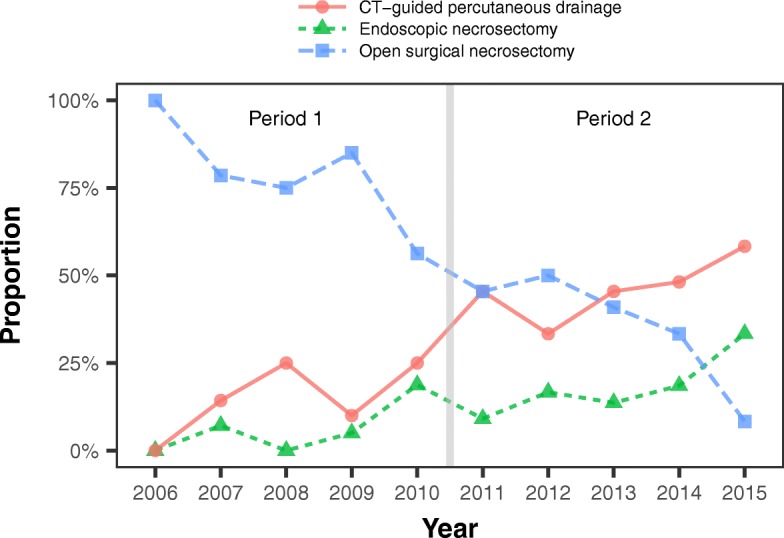
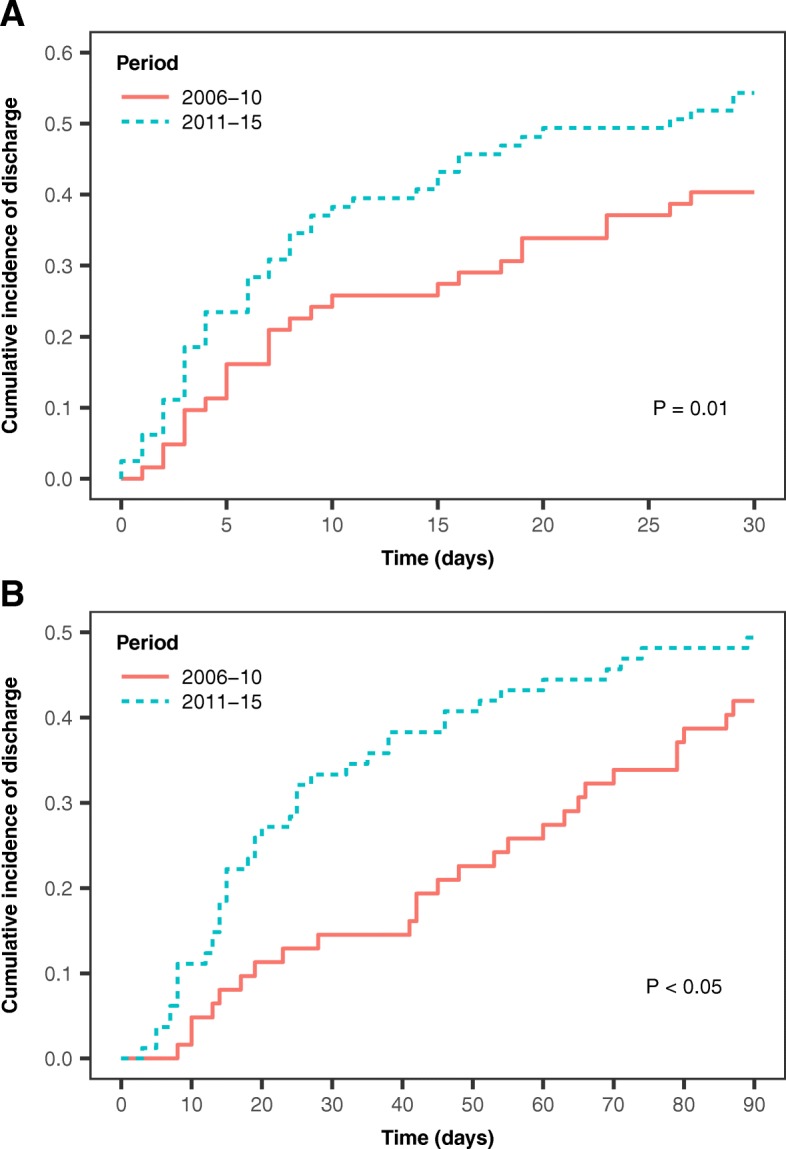
Surgical necrosectomy was more common in the early period (74% versus 41%; P <0.001), and use of minimally invasive drainage increased between the early and late periods (19% and 52%, respectively; P <0.001). The numbers of ventilator-free days and catecholamine-free days by day 30 were higher during the later period. The proportions of patients discharged from intensive care within the first 30 days and from the hospital within the first 90 days were higher during the second period. Hospital mortality was not significantly different between the early and late periods (19% and 22%, respectively).
In our study, the implementation of a minimally invasive drainage protocol in patients with infected pancreatic necrosis was associated with shorter times spent with organ dysfunction, in the intensive care unit, and in the hospital. Mortality was not significantly different. These results should be interpreted bearing in mind the limitations inherent in the before-after study design.
在因急性坏死性胰腺炎住院的患者中,约有 40%发生感染性胰腺坏死,需要联合使用抗生素治疗和局部引流。自 2010 年以来,开放式外科坏死切除术的引流已逐渐被经皮放射学引流、内镜坏死切除术和腹腔镜手术等微创方法所取代,这些方法在高度选择的患者的小随机对照试验中被证明是有效的。很少有研究评估在日常医院实践中使用微创引流方法的效果。本研究旨在确定与传统的开放式手术相比,微创引流是否能改善合并感染的急性坏死性胰腺炎重症患者的预后。
对因重症急性坏死性胰腺炎入住重症监护病房的患者进行单中心观察性研究,比较 2006 年 9 月至 2010 年 12 月期间主要采用传统开放式手术治疗的 62 例患者的特征、引流技术和结局,以及 2011 年 1 月至 2015 年 8 月引入微创引流方案后治疗的 81 例患者的特征、引流技术和结局。
早期外科坏死切除术更为常见(74%比 41%;P<0.001),微创引流的应用在早期和晚期之间有所增加(分别为 19%和 52%;P<0.001)。第 30 天无呼吸机天数和无儿茶酚胺天数更多。第二期内,30 天内从重症监护室出院和 90 天内从医院出院的患者比例更高。早期和晚期的院内死亡率无显著差异(分别为 19%和 22%)。
在本研究中,感染性胰腺坏死患者实施微创引流方案与器官功能障碍时间、入住重症监护病房时间和住院时间缩短有关。死亡率无显著差异。应考虑到前后研究设计固有的局限性来解释这些结果。