FIECON Ltd, 3 College Yard, Lower Dagnall Street, St Albans, Hertfordshire, AL3 4PA, UK.
Pharmacoeconomics. 2019 Mar;37(3):391-405. doi: 10.1007/s40273-018-0745-z.
The aim was to evaluate the cost-effectiveness of niraparib compared with routine surveillance (RS), olaparib and rucaparib for the maintenance treatment of patients with recurrent ovarian cancer (OC).
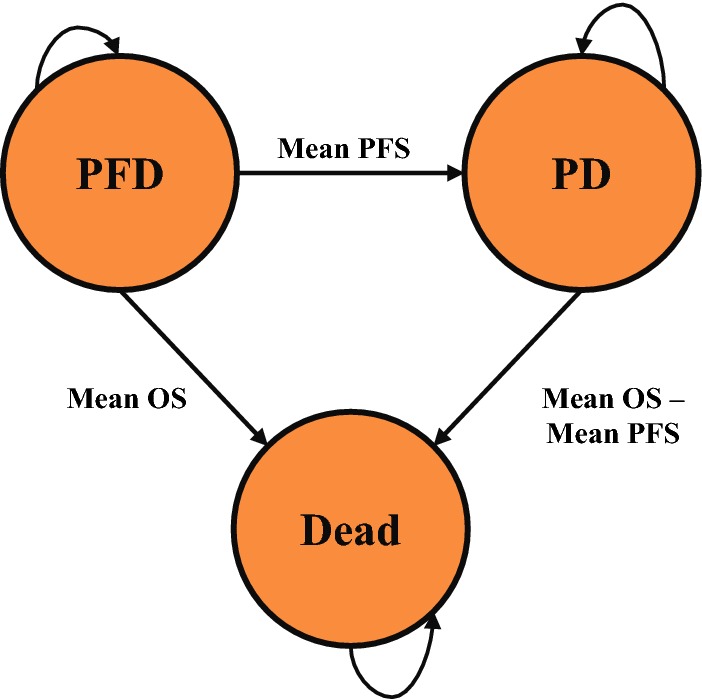
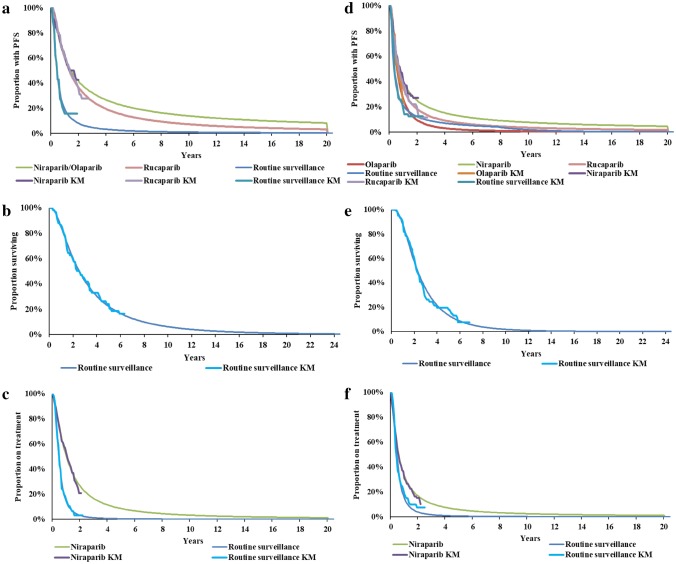
A decision-analytic model estimated the cost per quality-adjusted life-year (QALY) gained for niraparib versus RS, olaparib, and rucaparib from a US payer perspective. The model considered recurrent OC patients with or without germline BRCA mutations (gBRCAmut and non-gBRCAmut), who were responsive to their last platinum-based chemotherapy regimen. Model health states were: progression-free disease, progressed disease and dead. Mean progression-free survival (PFS) was estimated using parametric survival distributions based on ENGOT-OV16/NOVA (niraparib phase III trial), ARIEL3 (rucaparib phase III trial) and Study 19 (olaparib phase II trial). Mean overall survival (OS) benefit was estimated as double the mean PFS benefit based on the relationship between PFS and OS observed in Study 19. Costs included: drug, chemotherapy, monitoring, adverse events, and terminal care. EQ-5D utilities were estimated from trial data.
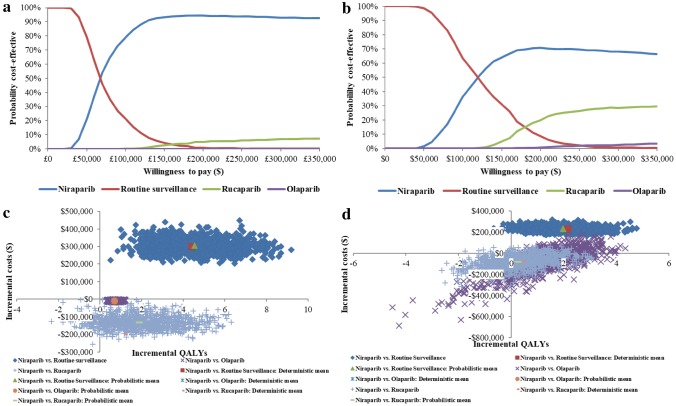
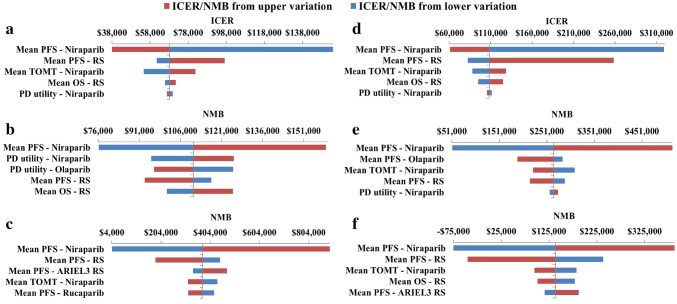
Compared to RS, niraparib was associated with an incremental cost-effectiveness ratio (ICER) of US$68,287/QALY and US$108,287/QALY for gBRCAmut and non-gBRCAmut, respectively. Compared to olaparib and rucaparib, niraparib decreased costs and increased QALYs, with a cost saving of US$8799 and US$22,236 versus olaparib and US$198,708 and US$73,561 versus rucaparib for gBRCAmut and non-gBRCAmut, respectively.
Niraparib was estimated to be less costly and more effective compared to olaparib and rucaparib, and the ICER fell within an acceptable range compared to RS. Therefore, niraparib may be considered a cost-effective maintenance treatment for patients with recurrent OC.
评估尼拉帕利相对于常规监测(RS)、奥拉帕利和鲁卡帕利用于复发性卵巢癌(OC)维持治疗的成本效果。
从美国支付者的角度,采用决策分析模型估算尼拉帕利相对于 RS、奥拉帕利和鲁卡帕利用于复发性 OC 患者的每质量调整生命年(QALY)成本。模型考虑了对末次铂类化疗有反应的复发性 OC 患者,无论其是否携带生殖系 BRCA 突变(gBRCAmut 和非 gBRCAmut)。模型健康状态为:无疾病进展、疾病进展和死亡。无进展生存期(PFS)的平均值使用基于 ENGOT-OV16/NOVA(尼拉帕利 III 期试验)、ARIEL3(鲁卡帕利 III 期试验)和 Study 19(奥拉帕利 II 期试验)的参数生存分布来估计。总生存(OS)获益的平均值估计为 PFS 获益的两倍,这是基于 Study 19 中观察到的 PFS 和 OS 之间的关系。成本包括:药物、化疗、监测、不良事件和终末期护理。EQ-5D 效用值从试验数据中估算。
与 RS 相比,gBRCAmut 和非 gBRCAmut 患者使用尼拉帕利的增量成本效果比(ICER)分别为 68287 美元/QALY 和 108287 美元/QALY。与奥拉帕利和鲁卡帕利相比,尼拉帕利降低了成本并增加了 QALYs,gBRCAmut 和非 gBRCAmut 患者相对于奥拉帕利分别节省了 8799 美元和 22236 美元,相对于鲁卡帕利分别节省了 198708 美元和 73561 美元。
与奥拉帕利和鲁卡帕利相比,尼拉帕利估计成本更低、效果更好,与 RS 相比,ICER 在可接受范围内。因此,尼拉帕利可能被视为复发性 OC 患者的一种具有成本效果的维持治疗。