Global Health Cluster, Division for Health Services, Norwegian Institute of Public Health, Oslo, Norway.
Centre for Intervention Science in Maternal and Child Health (CISMAC), University of Bergen, Bergen, Norway.
PLoS One. 2018 Nov 27;13(11):e0207813. doi: 10.1371/journal.pone.0207813. eCollection 2018.
In most low- and middle-income settings, national aggregate health data is the most consistently available source for policy-making and international comparisons. In the West Bank, the paper-based health information system with manual aggregations is transitioning to an individual-level data eRegistry for maternal and child health at the point-of-care. The aim of this study was to explore beforehand how routine health information systems indicators for antenatal care can change with the introduction of the eRegistry.
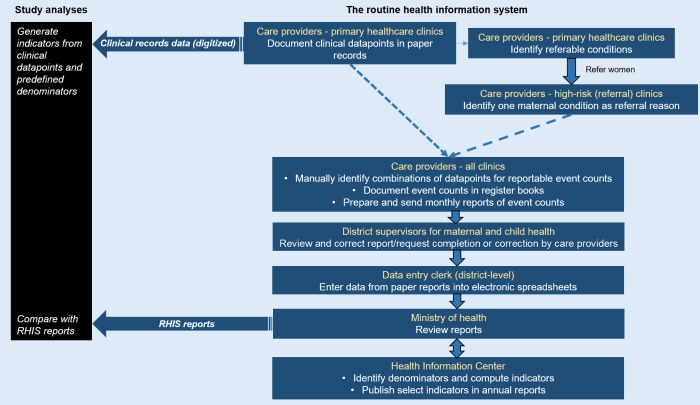
Data were collected from clinical antenatal paper records of pregnancy enrollments for 2015 from 17 primary healthcare clinics, selected by probability sampling from five districts in the West Bank. We used the individual-level data from clinical records to generate routinely reported health systems indicators. We weighted the data to produce population-level estimates, and compared these indicators with aggregate routine health information systems reports.
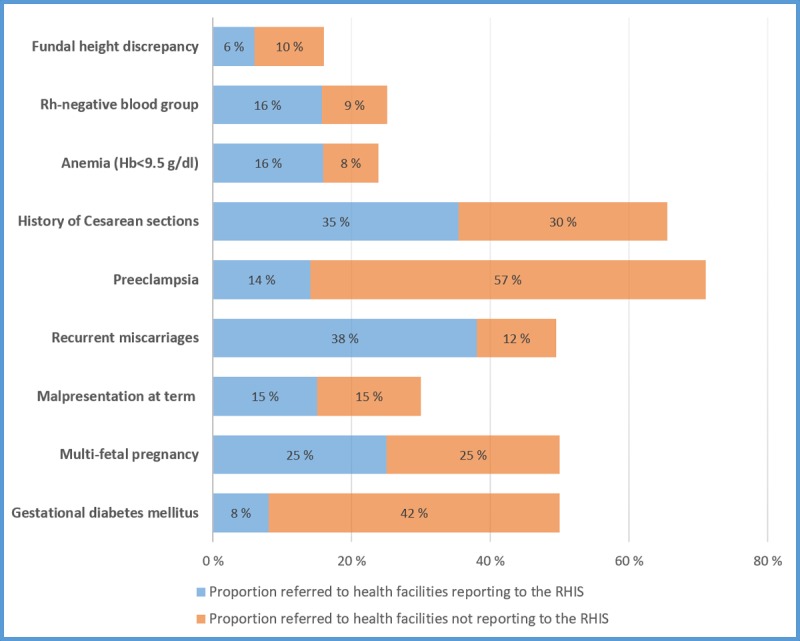
Antenatal anemia screening at 36 weeks was 20% according to the clinical records data, compared to 52% in the routine reports. The clinical records data showed considerably higher incidences of key maternal conditions compared to the routine reports, including fundal height discrepancy (20% vs. 0.01%); Rh-negative blood group (6.8% vs. 1.4%); anemia with hemoglobin<9.5 g/dl (6% vs. 0.6%); and malpresentation at term (1.3% vs. 0.03%). Only about a sixth of cases with these conditions were referred according to guidelines to designated referral clinics.
Differences between indicators from the clinical records data and routine health information systems reports can be attributed to human error, inconsistent denominators, and complexities of data processes. Key health systems indicators were prone to underestimations since their registration was dependent on referral of pregnant women. With a transition to individual-level data, as in the eRegistry under implementation, the public health authorities will be able to generate reliable health systems indicators reflective of the population's health status.
在大多数低收入和中等收入国家,国家综合健康数据是政策制定和国际比较最常用的来源。在约旦河西岸,基于纸质的、手动汇总的卫生信息系统正在向在护理点获取母婴健康的个人层面电子登记册过渡。本研究旨在预先探讨在引入电子登记册后,产前护理常规卫生信息系统指标如何发生变化。
数据来自 2015 年五个地区的 17 个初级保健诊所中通过概率抽样选择的妊娠登记的临床产前纸质记录。我们使用临床记录中的个人层面数据来生成常规报告的卫生系统指标。我们对数据进行加权以产生人群水平的估计,并将这些指标与汇总的常规卫生信息系统报告进行比较。
根据临床记录数据,36 周的产前贫血筛查率为 20%,而常规报告中的这一比例为 52%。临床记录数据显示,关键产妇情况的发生率明显高于常规报告,包括宫底高度差异(20%比 0.01%);Rh 阴性血型(6.8%比 1.4%);血红蛋白<9.5g/dl 的贫血(6%比 0.6%);足月胎位不正(1.3%比 0.03%)。根据指南,只有大约六分之一的这些病例被转诊到指定的转诊诊所。
临床记录数据和常规卫生信息系统报告中的指标差异可归因于人为错误、不一致的分母和数据处理的复杂性。由于孕妇的转诊依赖于关键卫生系统指标的注册,因此这些指标容易被低估。随着向电子登记册等个人层面数据的过渡,公共卫生当局将能够生成反映人口健康状况的可靠卫生系统指标。