Cancer Research UK & UCL Cancer Trials Centre, UCL Cancer Institute, University College London, London, UK.
Freeman Hospital, Newcastle upon Tyne, UK.
Lancet Diabetes Endocrinol. 2019 Jan;7(1):44-51. doi: 10.1016/S2213-8587(18)30306-1. Epub 2018 Nov 27.
Two large randomised trials of patients with well-differentiated thyroid cancer reported in 2012 (HiLo and ESTIMABL1) found similar post-ablation success rates at 6-9 months between a low administered radioactive iodine (I) dose (1·1 GBq) and the standard high dose (3·7 GBq). However, recurrence rates following radioactive iodine ablation have previously only been reported in observational studies, and recently in ESTIMABL1. We aimed to compare recurrence rates between radioactive iodine doses in HiLo.
HiLo was a non-inferiority, parallel, open-label, randomised controlled factorial trial done at 29 centres in the UK. Eligible patients were aged 16-80 years with histological confirmation of differentiated thyroid cancer requiring radioactive iodine ablation (performance status 0-2, tumour stage T1-T3 with the possibility of lymph-node involvement but no distant metastasis and no microscopic residual disease, and one-stage or two-stage total thyroidectomy). Patients were randomly assigned (1:1:1:1) to 1·1 GBq or 3·7 GBq ablation, each prepared with either recombinant human thyroid-stimulating hormone (rhTSH) or thyroid hormone withdrawal. Patients were followed up at annual clinic visits. Recurrences were diagnosed at each hospital with a combination of established methods according to national standards. We used Kaplan-Meier curves and hazard ratios (HRs) for time to first recurrence, which was a pre-planned secondary outcome. This trial is registered with ClinicalTrials.gov, number NCT00415233.
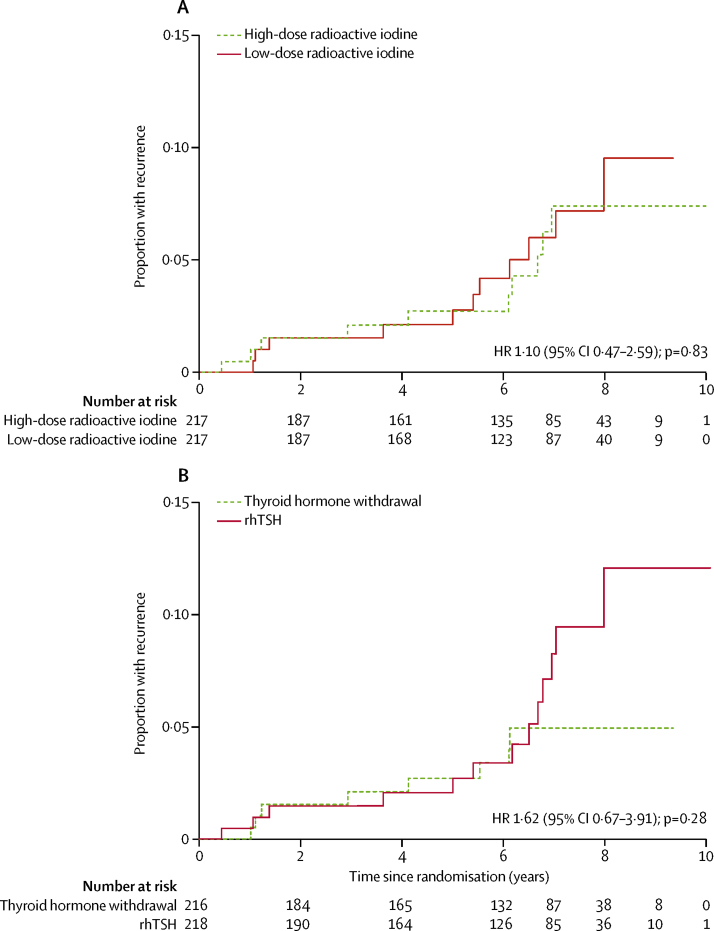
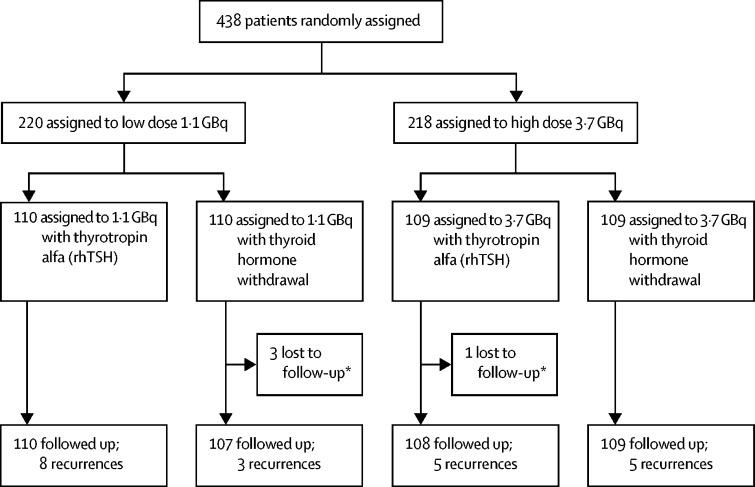
Between Jan 16, 2007, and July 1, 2010, 438 patients were randomly assigned. At the end of the follow-up period in Dec 31, 2017, median follow-up was 6·5 years (IQR 4·5-7·6) in 434 patients (217 in the low-dose group and 217 in the high-dose group). Confirmed recurrences were seen in 21 patients: 11 who had 1·1 GBq ablation and ten who had 3·7 GBq ablation. Four of these (two in each group) were considered to be persistent disease. Cumulative recurrence rates were similar between low-dose and high-dose radioactive iodine groups (3 years, 1·5% vs 2·1%; 5 years, 2·1% vs 2·7%; and 7 years, 5·9% vs 7·3%; HR 1·10 [95% CI 0·47-2·59]; p=0·83). No material difference in risk was seen for T3 or N1 disease. Recurrence rates were also similar among patients who were prepared for ablation with rhTSH and those prepared with thyroid hormone withdrawal (3 years, 1·5% vs 2·1%; 5 years, 2·1% vs 2·7%; and 7 years, 8·3% vs 5·0%; HR 1·62 [95% CI 0·67-3·91]; p=0·28). Data on adverse events were not collected during follow-up.
The recurrence rate among patients who had 1·1 GBq radioactive iodine ablation was not higher than that for 3·7 GBq, consistent with data from large, recent observational studies. These findings provide further evidence in favour of using low-dose radioactive iodine for treatment of patients with low-risk differentiated thyroid cancer. Our data also indicate that recurrence risk was not affected by use of rhTSH.
Cancer Research UK.
2012 年发表的两项大型随机试验(HiLo 和 ESTIMABL1)报告了分化型甲状腺癌患者的术后消融成功率,在低剂量放射性碘(I)(1.1GBq)和标准高剂量(3.7GBq)之间,6-9 个月时的成功率相似。然而,此前仅在观察性研究中报告了放射性碘消融后的复发率,最近在 ESTIMABL1 中也有报告。我们旨在比较 HiLo 中两种放射性碘剂量之间的复发率。
HiLo 是在英国 29 个中心进行的一项非劣效性、平行、开放性、随机对照因子试验。合格的患者年龄为 16-80 岁,经组织学证实患有需要放射性碘消融的分化型甲状腺癌(表现状态 0-2,肿瘤分期 T1-T3,可能有淋巴结受累,但无远处转移和无显微镜下残留疾病,以及一期或二期全甲状腺切除术)。患者随机分为 1.1GBq 或 3.7GBq 消融组,每组分别用重组人促甲状腺激素(rhTSH)或甲状腺激素停药准备。患者每年在门诊就诊。复发在每个医院根据国家标准采用多种已建立的方法进行诊断。我们使用 Kaplan-Meier 曲线和风险比(HR)来评估首次复发的时间,这是一项预先计划的次要结局。该试验在 ClinicalTrials.gov 上注册,编号为 NCT00415233。
在 2007 年 1 月 16 日至 2010 年 7 月 1 日期间,共纳入 438 名患者。在 2017 年 12 月 31 日的随访结束时,434 名患者的中位随访时间为 6.5 年(IQR 4.5-7.6),其中 217 名患者接受低剂量组消融,217 名患者接受高剂量组消融。在 21 名患者中发现了确诊的复发:11 名接受了 1.1GBq 消融,10 名接受了 3.7GBq 消融。其中 4 名(每组 2 名)被认为是持续性疾病。低剂量和高剂量放射性碘组的累积复发率相似(3 年时为 1.5% vs 2.1%;5 年时为 2.1% vs 2.7%;7 年时为 5.9% vs 7.3%;HR 1.10 [95%CI 0.47-2.59];p=0.83)。T3 或 N1 疾病的风险没有明显差异。rhTSH 准备消融和甲状腺激素停药准备消融的患者之间的复发率也相似(3 年时为 1.5% vs 2.1%;5 年时为 2.1% vs 2.7%;7 年时为 8.3% vs 5.0%;HR 1.62 [95%CI 0.67-3.91];p=0.28)。在随访期间没有收集不良事件的数据。
接受 1.1GBq 放射性碘消融的患者的复发率并不高于接受 3.7GBq 放射性碘消融的患者,这与最近的大型观察性研究数据一致。这些发现进一步支持使用低剂量放射性碘治疗低危分化型甲状腺癌患者。我们的数据还表明,复发风险不受 rhTSH 使用的影响。
英国癌症研究中心。