Choi Kyung Hwa, Jeon Jeong Yong, Lee Young-Eun, Kim Seung Won, Kim Sang Yong, Yun Yeo Jin, Park Ki Cheong
Department of Urology, CHA Bundang Medical Center, CHA University, Seongnam 463-712, Republic of Korea.
Brain Korea 21 Project for Medical Science, Yonsei University College of Medicine, Seoul 120-752, South Korea; Department of Nuclear medicine, Yonsei University College of Medicine, 50-1, Yonsei-ro, Seodaemun-gu, Seoul, 120-752, Republic of Korea.
Transl Oncol. 2019 Feb;12(2):381-388. doi: 10.1016/j.tranon.2018.11.007. Epub 2018 Dec 3.
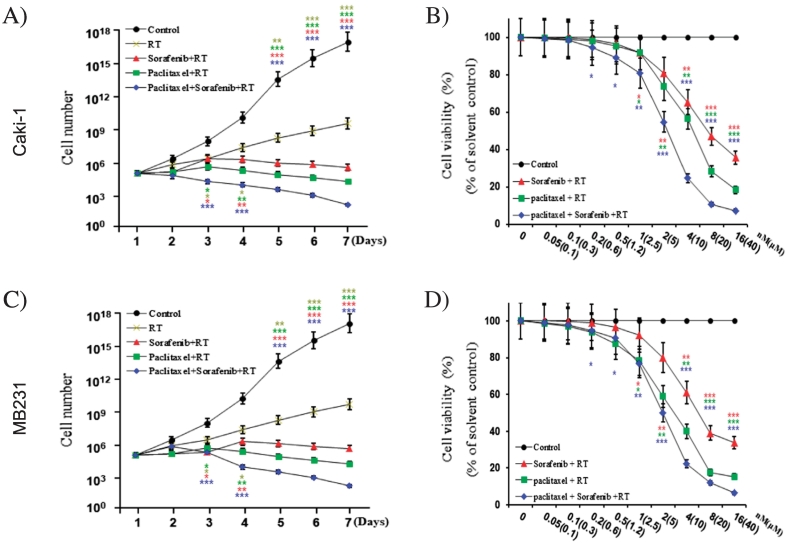
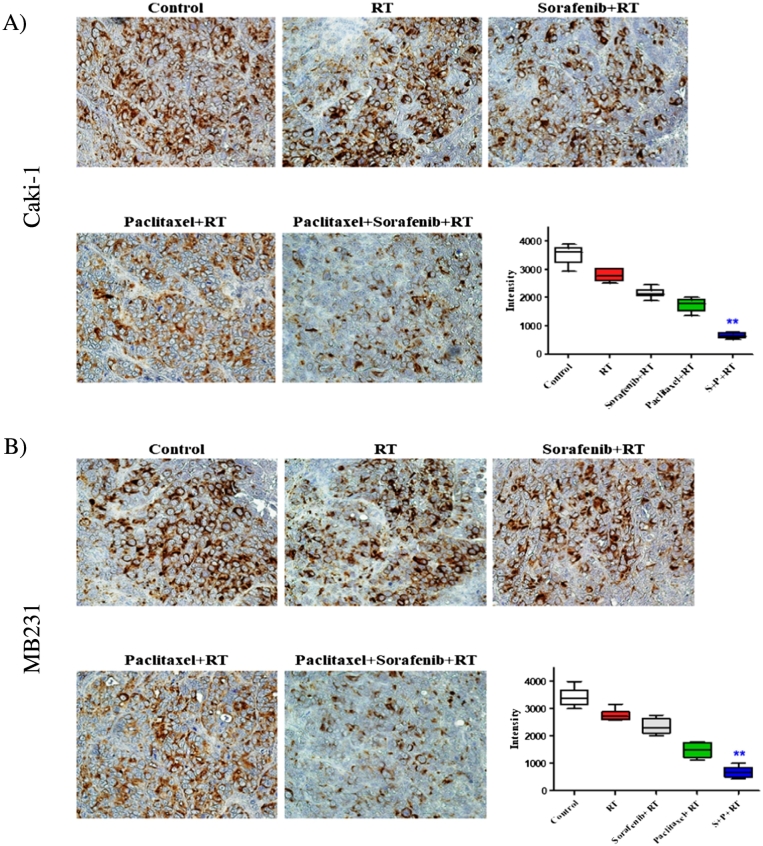
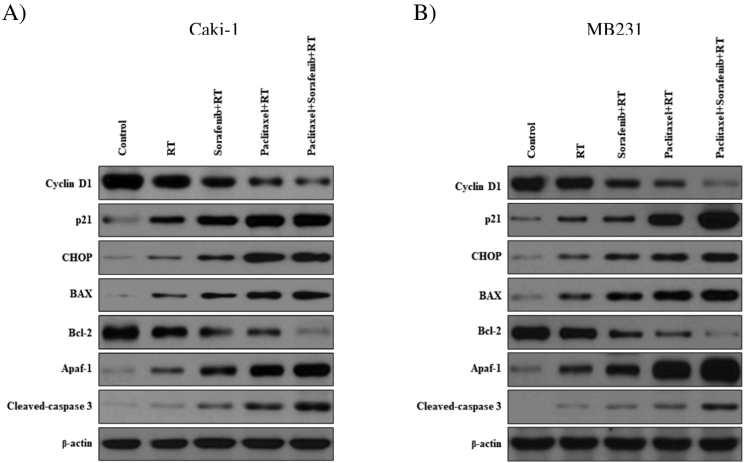
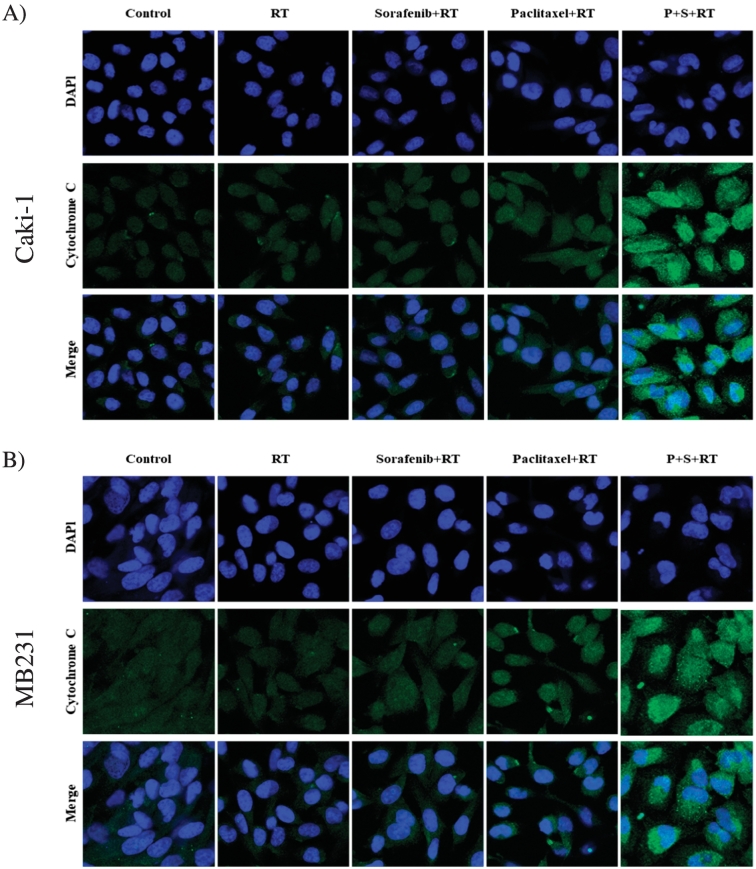
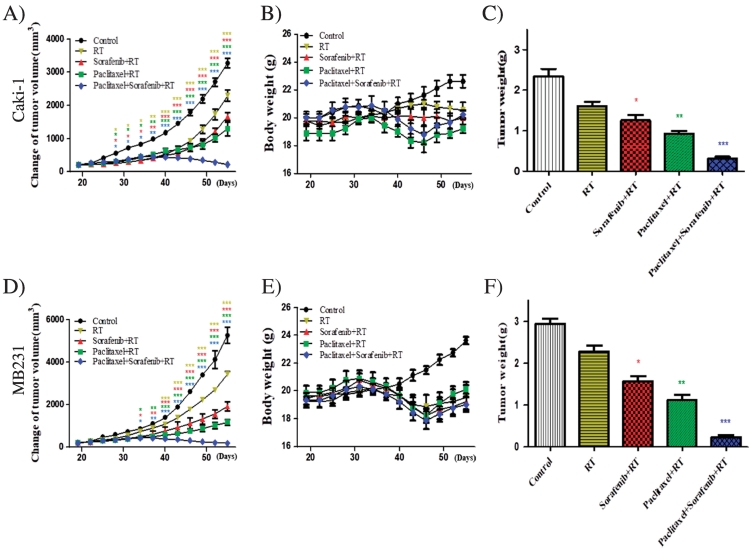
Advanced cancer has been shown to be associated with a higher percentage of epigenetic changes than with genetic mutations. Preclinical models have shown that the combination of paclitaxel, sorafenib, and radiation therapy (RT) plays a crucial role in renal cell carcinoma (RCC) and breast cancer. This study aimed to investigate the involvement of mitochondrial cytochrome c-dependent apoptosis in the mechanism of action of a combination of paclitaxel, sorafenib, and RT in RCC and breast cancer. RCC and breast cancer cell lines were exposed to paclitaxel and sorafenib alone or combined in the presence of radiation, and cell viability was determined using the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide assay. The synergistic anticancer effects of the combination therapy on cell cycle and intracellular signaling pathways were estimated using flow cytometry and immunoblot analysis. RCC and breast cancer cell line xenograft models were used to examine the antitumor activity in vivo. Our results suggest that paclitaxel, sorafenib, and RT synergistically decreased the viability of RCC and breast cancer cells and significantly induced their apoptosis, as shown by caspase-3 cleavage. Paclitaxel, sorafenib, and radiation cotreatment reduced antiapoptotic factor levels in these cells and, thereby, significantly reduced the tumor volume of RCC and breast cancer cell xenografts. The current study suggests that paclitaxel, sorafenib, and radiation cotreatment was more effective than cotreatment with paclitaxel or sorafenib and radiation. These findings may offer a new therapeutic approach to RCC and breast cancer.
研究表明,与基因突变更常见于早期癌症不同,晚期癌症中表观遗传变化的比例更高。临床前模型表明,紫杉醇、索拉非尼和放射治疗(RT)联合使用在肾细胞癌(RCC)和乳腺癌治疗中发挥关键作用。本研究旨在探讨线粒体细胞色素c依赖性凋亡在紫杉醇、索拉非尼和RT联合治疗RCC和乳腺癌作用机制中的参与情况。将RCC和乳腺癌细胞系单独或联合暴露于紫杉醇和索拉非尼,并在有辐射的情况下进行处理,使用3-(4,5-二甲基噻唑-2-基)-2,5-二苯基四氮唑溴盐法测定细胞活力。使用流式细胞术和免疫印迹分析评估联合治疗对细胞周期和细胞内信号通路的协同抗癌作用。使用RCC和乳腺癌细胞系异种移植模型来检测体内抗肿瘤活性。我们的结果表明,紫杉醇、索拉非尼和RT联合使用可协同降低RCC和乳腺癌细胞的活力,并显著诱导其凋亡,如半胱天冬酶-3的裂解所示。紫杉醇、索拉非尼和放射联合治疗降低了这些细胞中的抗凋亡因子水平,从而显著减小了RCC和乳腺癌细胞异种移植瘤的体积。当前研究表明,紫杉醇、索拉非尼和放射联合治疗比紫杉醇或索拉非尼与放射联合治疗更有效。这些发现可能为RCC和乳腺癌提供一种新的治疗方法。