HealthCore, Inc., Wilmington, DE, USA.
Eli Lilly and Company, Indianapolis, IN, USA.
Adv Ther. 2019 Jan;36(1):118-130. doi: 10.1007/s12325-018-0828-4. Epub 2018 Dec 7.
Complex or personalized insulin regimens challenge traditional adherence measures. Our objective was to develop an improved basal insulin (BI) adherence measure using both patient-reported and administrative claims data, resulting in a more complete measure.
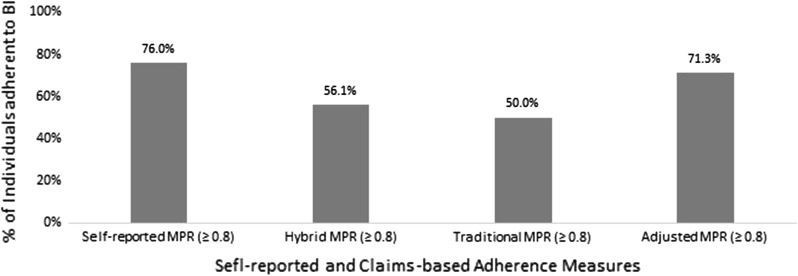
Patients' self-reported BI utilization over the previous 12 months was linked with their claims data for the same period. Hybrid medication possession ratio (MPR) was derived by calculating expected days of insulin supply [total dispensed insulin units from claims over 12 months divided by self-reported total daily dose (TDD)]. The hybrid MPR was compared against traditional claims-based MPR, adjusted claims-based MPR, and patient-reported MPR. For all MPR measures, the adherence threshold was ≥ 0.8. A logistic model was used to predict non-adherence per hybrid MPR. The predicted model-based MPR was compared with existing measures in a larger cohort.
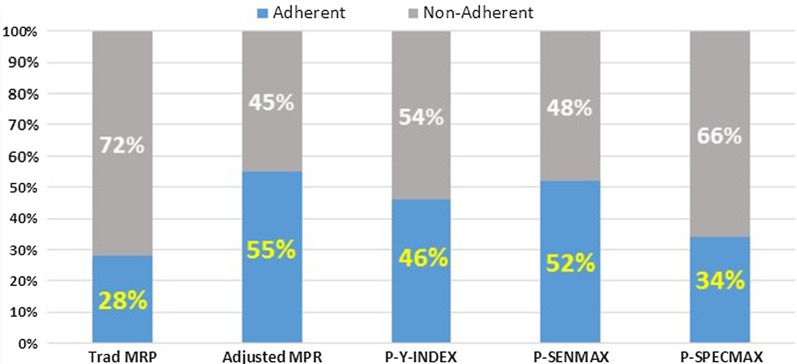
The study sample consisted of 296 patients. TDD derived from claims was higher than self-reported TDD [77.9 (71.8) vs. 57.7 (38.3)], implying average dispensed insulin would last longer than claims-based days supply. Correspondingly, hybrid and MPRs adjusted for package size (56% and 71%, respectively) were higher than claims-based MPR (50%). Age, total claims-based days supply, retinopathy, adjusted MPR-based adherence, and non-insulin injectable use were key predictors of hybrid MPR-based adherence. Applying the claims-based prediction model to a larger cohort to test validity showed high correlations with predicted and adjusted MPR-based adherence.
Traditional claims-based MPR underestimated adherence while adjusted MPR overestimated adherence when self-reported total daily dose was taken as benchmark insulin dose. The predicted model may help identify patients with poor basal insulin adherence. More research is needed to further confirm the findings.
Eli Lilly and Company, Indianapolis, IN, USA.
复杂或个性化的胰岛素治疗方案给传统的依从性测量带来了挑战。我们的目标是利用患者报告和行政索赔数据开发一种改进的基础胰岛素(BI)依从性测量方法,从而得到一个更完整的测量方法。
将患者在过去 12 个月内自我报告的 BI 使用情况与同期的索赔数据相联系。混合药物使用比例(MPR)通过计算预期的胰岛素供应天数[从索赔中获得的 12 个月内总胰岛素单位数除以自我报告的总日剂量(TDD)]得出。混合 MPR 与传统的基于索赔的 MPR、调整后的基于索赔的 MPR 和患者报告的 MPR 进行了比较。对于所有 MPR 测量方法,依从性阈值均≥0.8。使用逻辑模型预测每一个混合 MPR 的不依从性。将预测模型基础 MPR 与更大队列中的现有指标进行比较。
研究样本包括 296 名患者。从索赔中得出的 TDD 高于自我报告的 TDD[77.9(71.8)比 57.7(38.3)],这意味着平均开出的胰岛素比基于索赔的供应天数持续时间更长。相应地,调整了包装尺寸的混合 MPR(56%和 71%)和 MPR(50%)均高于基于索赔的 MPR。年龄、总基于索赔的供应天数、视网膜病变、调整后的基于 MPR 的依从性和非胰岛素注射剂的使用是混合 MPR 基于依从性的关键预测因素。将基于索赔的预测模型应用于更大的队列中进行验证,结果表明与预测和调整后的基于 MPR 的依从性高度相关。
当以自我报告的总日剂量为基准胰岛素剂量时,传统的基于索赔的 MPR 低估了依从性,而调整后的 MPR 则高估了依从性。预测模型可能有助于识别基础胰岛素依从性差的患者。还需要进一步的研究来进一步证实这些发现。
美国印第安纳州印第安纳波利斯市礼来公司。